
Randomized controlled trials of pain control measures prior to planned painful procedures that have an untreated control group are unethical.
I would have thought in 2022 that statement was about as uncontroversial as a statement about ethics could be, nevertheless such studies continue to be performed and published.
In one of my recent posts I wrote about an article in the journal “Pain” where a group of babies were randomized to experience pain. I wrote to the editor about my concerns and was asked to write a “letter to the editor”, which I did.
The text of the letter is here:
The article, by Gao et al [3], Effect of combined pharmacological, behavioral, and physical interventions for procedural pain on salivary cortisol and neurobehavioral development in preterm infants: a randomized controlled trial,” published in your journal describes a research project which is clearly unethical[1] and should not have been published.
In this study, newborn babies were assigned to a group designed to experience repeated painful interventions. The express purpose of the design was to create a group of newborn infants who had repeated, avoidable pain. The control group had a mean of 35 painful procedures per baby (SD 15), with mean PIPP scores indicating moderate to severe pain. Pain which could easily have been dramatically reduced or completely avoided.
This research is clearly in conflict with the declaration of Helsinki[6], which notes that untreated controls should only be included in a trial “in the absence of existing proven therapy”, whereas there is an abundance of existing proven therapies for the procedures studied in this trial, from randomized controlled trials involving many thousands of newborn infants. Effective methods to prevent pain caused by skin-breaking procedures are well known, easily available, and cheap or free. Those methods include kangaroo care/skin-to-skin contact, oral sucrose or glucose solutions, especially when combined with non-nutritive sucking, and breastfeeding. There is no valid reason for denying such pain reduction methods to research subjects. Publication in a high-quality journal such as Pain gives credibility to the research and suggests that it is acceptable to inflict pain on babies in order to complete a research project.
Research which compares an analgesic intervention for a painful procedure in newborn infants to an untreated control group is useless in improving care. As effective pain measures are already well known, the only research which could possibly improve care is that which compares different analgesic interventions, or examines the addition of measures to those already known to be effective. It is already clear that repeated painful procedures, as studied in this trial, have adverse effects on stress, neurological and developmental outcomes[5]. It is further already known that routine analgesic interventions mitigate these adverse effects; as a result, national[2] and international[4] guidelines require that analgesia is used for all painful procedures in newborn infants.
The most effective way your journal could improve pain control in newborn infants would be to cease publishing research which unethically randomizes babies to have avoidable pain. All future trials in newborn infants undergoing planned painful procedures that the journal publishes should ensure that all the babies receive proven effective methods of pain control.
I urge you to consider withdrawing this article, and to establish editorial guidelines which prevent the publication of research which imposes avoidable pain on the participants. Specifically, studies comparing pain responses in newborn infants which include an untreated control group should never be published.
The letter was sent out to referees, I guess the same ones who refereed the initial publication, I don’t know as it was all anonymous, referee numbers 1 and 2 had similar points in responses to my letter: They both made the point that the procedures were required for clinical care, that was not in dispute, and has no relevance to my arguments. Referee 2 made the following point:
The article by Gao and colleagues state that it is routine in the unit where the study took place for pain-relieving interventions to be administered once a baby starts crying rather than before. If this RCT had not been conducted, then all the babies in this study would have received this form of care.
Similar comments were made by referee 1, in other words, they are saying that the fact that pain is so badly handled, in this NICU and in many others, is sufficient justification for not providing effective analgesia in the trial. Waiting for the baby to demonstrate that they are in pain, and then trying to soothe them afterwards, is, according to these reviewers, acceptable as a method of pain control. There is, of course, a huge literature showing that pre-emptive pain control, prior to painful procedures, is much more effective than after the fact; waiting for the baby to be in pain, then trying to calm them down afterwards, is completely inadequate as an approach to painful interventions. Just because the NICU does not currently follow adequate pain control standards is not a good reason for publishing a trial comparing their inadequate usual approach to something else.
One of the referees of my letter also notes that it has been stated that neonatal providers in China need a high-quality, evidence-based guideline for the treatment and management of neonatal pain. Which may well be true, but that does not justify performing research on Chinese babies which inflicts avoidable pain. There is already enough published data about pain responses without hurting Chinese babies too.
As you might guess from this post, the editor rejected my letter, which I think shows a certain cowardice, they should at least let the readers consider the arguments for themselves.
One of the referees of the letter actually gives references to 2 articles and a registered protocol which come from a single group. In all of those references there are babies receiving planned painful skin breaking procedures without analgesia, which leads me to guess that there is some auto-justification going on here, and that perhaps this referee has been performing similar unethical studies. When I looked at one of those studies, published as correspondence in a non-paediatric journal (Gursul D, et al. Stroking modulates noxious-evoked brain activity in human infants. Curr Biol. 2018 Dec 17;28(24):R1380-R1381), I was appalled to find that the first of 2 studies, briefly reported together, inflicted pain for no valid reason at all. They took 30 full term infants and gave them pain using a pinprick stimulator and measured the EEG responses, showing noxious related EEG changes in the control babies who received no analgesic intervention. The principal investigator of that study has published articles suggesting that behavioural pain responses are not very important, and that we should use EEG noxious changes as the method to detect pain in newborns. I disagree with that contention, but even if you accept that argument, how does one justify creating pain in otherwise healthy normal babies by sticking needles into them, and “proving” that they have pain using an EEG, without any clinical justification for the pain? This is one of the least ethical studies I have seen in recent years in newborn infants. This part of the study was a comparison between pain from pinpricks with either no analgesic intervention or stroking the leg with a brush, in a specific fashion thought to stimulate C-fibres. The heels of the babies were pricked 27 times in 3 blocks, which appears to be in order to average out the EEG background changes so the the noxious related waves can be seen. I have to admit that this seems to be a relatively mild painful stimulus, the babies usually pulled their legs away, but in similar previous studies this group has shown that the pain they administer with this system is not enough to increase PIPP scores, even though they see EEG changes and the baby withdraws their leg.
In the second part of that letter (Gursul et al) they report a study which appears to be not randomized (it is so poorly reported that it is not clear how the babies were divided into intervention and control groups, at one point they say the controls were “age-matched” but the intervention group was 5 days old and the controls were 2.5 days), the babies had a heel poke for some clinically required blood work, and the (either14 or 16) controls had no analgesic intervention, the 20 in the intervention group had the brushing intervention thought to stimulate C-fibres, which, in 16 of them, decreased the EEG changes and shortened the duration of facial grimacing (they did not do formal assessment on a pain scale). The controls were therefore assigned to a group designed to have pain, with no pre-emptive analgesia, and without even any evidence that they had calming procedures after the heel poke when they were crying.
Other new publications to add to the list of shame include Talebi M, et al. The effect of concurrent use of swaddle and sucrose on the intensity of pain during venous blood sampling in neonate: a clinical trial study. BMC Pediatr. 2022;22(1):263, which studied 4 groups, swaddling, sucrose, combined sucrose and swaddling and nothing at all. Not surprisingly, nothing at all was worse than any of the other interventions, and that control group was completely unnecessary and subjected to avoidable pain.
Another study shows that you can do such research without an untreated control group, and have useful results. They compared breastfeeding to 20% glucose to non-nutritive sucking prior to a clinically required heel-poke, and did not have an untreated group. (Napiórkowska-Orkisz M, et al. Evaluation of Methods to Minimize Pain in Newborns during Capillary Blood Sampling for Screening: A Randomized Clinical Trial. Int J Environ Res Public Health. 2022;19(2):870), I would argue that NNS without glucose is already known to have a somewhat limited efficacy, but this smallish study (n=30 per group) did not show much difference between groups; as a very positive note, they mention in the introduction that they did not have an untreated control group for ethical reasons.
A new systematic review has examined the role of NNS in combination with sucrose, and shows that there is a consistently better control of pain with the combination than with either alone. (Li Q, et al. Efficacy and safety of combined oral sucrose and nonnutritive sucking in pain management for infants: A systematic review and meta-analysis. PLoS One. 2022;17(5):e0268033)
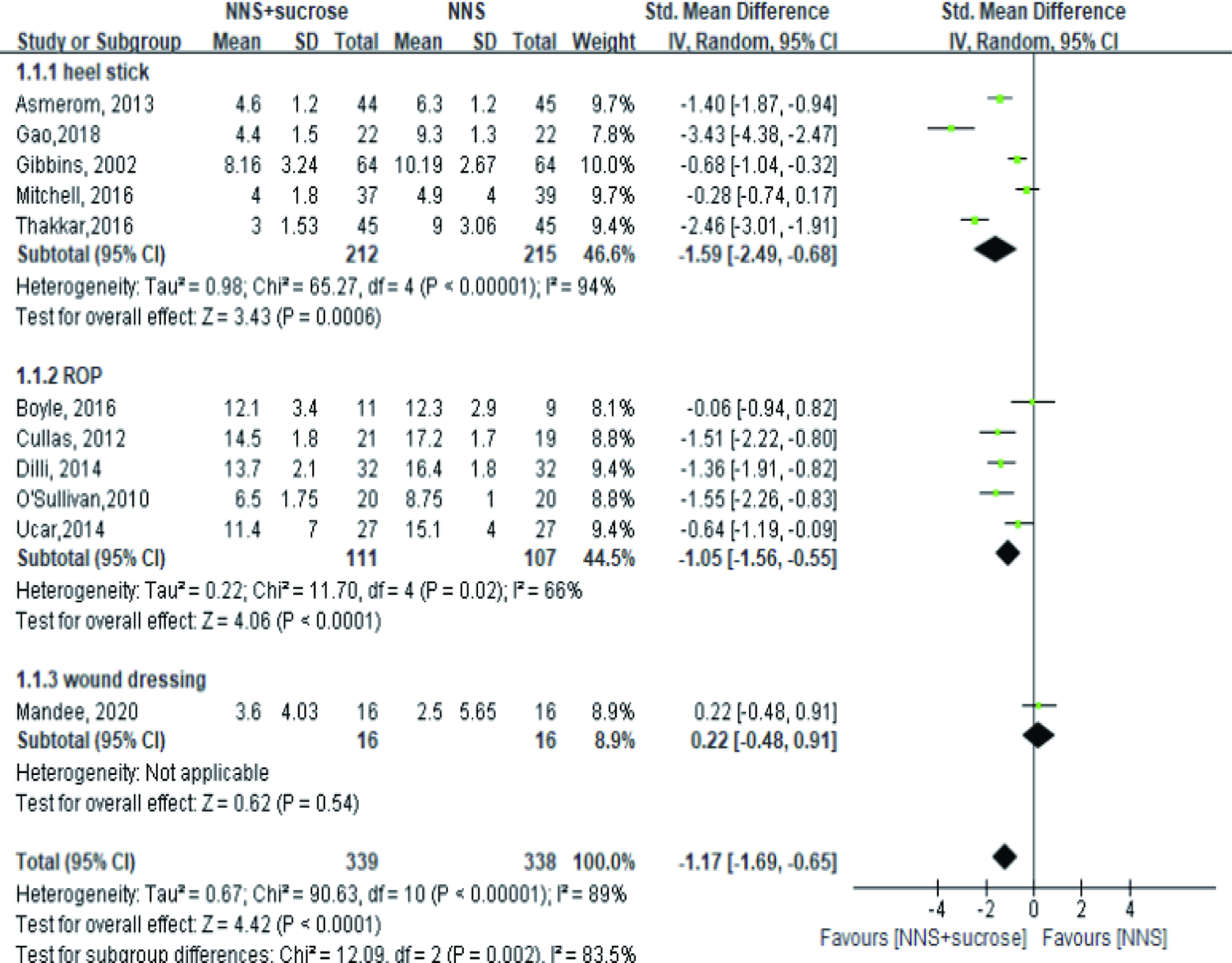
Most of these studies used the PIPP score, if you take out the Mandee study, and O’Sullivan, which used different scales, and should not be analyzed together, the results are similar, with better pain control during heel sticks, and slightly better pain scores during RoP screening, but as you can see from the mean scores, RoP screening still leads to high PIPP scores (means of 12 to 17) even with the combined intervention.
This review also compared combined NNS and sucrose to breastmilk or breastfeeding, but found very little data, 1 study of heelstick comparing NNS and sucrose to breast feeding and 1 of venepuncture comparing the combination to expressed breast milk, both showing similar pain control.
This review supports the idea that the optimal analgesia, prior to heel pokes, if the mother is not present, is a combination of sucrose and a soother; breast milk might be as effective, but there is less data. If mum is there, then breastfeeding for babies when that is appropriate, or skin to skin care, may be about as effective, and if dad is present then skin to skin care by him might also work, but I am having difficulty finding data about that.






