
Just after I pressed “post” for a recent addition to the blog, I saw this appear. (Callahan KP, et al. Influence of Genetic Information on Neonatologists’ Decisions: A Psychological Experiment. Pediatrics. 2022;149). It illustrates some major problems in how neonatologists react to genetic information. The authors questioned a national sample of neonatologists about how they would react to some genetic information. The respondents were randomized and each received 4 clinical vignettes, either with or without some genetic information, the cases were designed to illustrate real dilemmas that we face in clinical practice. One case that was really concerning was concerning an extremely preterm infant with an unusually protracted resolution of his lung disease in whom whole exome sequencing had been performed, in one version of the case there was no diagnostic abnormality, in the other the sequencing revealed homozygous abnormality of uncertain significance in a surfactant protein gene.
I would have thought that a finding of “uncertain significance” should have no impact on treatment approaches or goals, but that is not what was found.
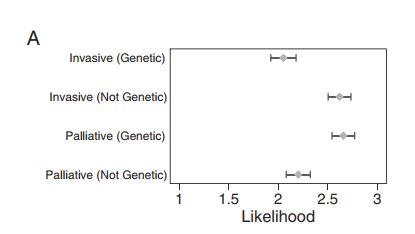
For this scenario, that figure shows that neonatologists who got the information that there was a variant of uncertain significance (“Genetic”) were more likely to desire palliative care, and less likely to recommend invasive interventions than those who were told the WGS was normal (“Not Genetic”).
My interpretation of the finding is that many neonatologists do not understand what a variant of “uncertain significance” means, and that we are in need of education.
The American College of Medical Genetics classifies genetic variants into 5 groups: pathogenic; likely pathogenic; of uncertain significance; likely benign or benign. The terminology “variant of uncertain significance” is used for situations where the variant is either previously unreported or there are not enough cases to know what the impact might be. Sometimes the genetic geniuses can guess that, for example, a mutation which leads to an early stop codon, in an essential gene with other known diseases associated, is likely to be pathogenic, even if it has never been seen before. But a variant of unknown significance could easily be a mutation with no clinical impact at all. Surely a variant of uncertain significance should have no impact on decision-making.
The discussion of this case is very illuminating : “For this case, respondents cited pain and suffering as more important considerations if they saw the genetic version of the case and were thus more likely to recommend palliative care. There is no reason to believe that a VUS would be associated with increased pain and suffering. This pattern is in line with previous work documenting that physicians cite quality of life more often when recommending palliative, rather than invasive, interventions. It is also consistent with reported use of suffering to represent the general utility of an intervention and justify a wide variety of decisions.”
That is certainly also my experience, when neonatologists think that we should continue intensive care we talk about chances of survival and long term outcomes, when we want to limit care we start talking about suffering. I don’t understand though why a VUS (variant of unknown significance) would have any impact on those considerations.
In another of the cases there was an incidental finding of William’s syndrome in an extreme preterm baby at 2 weeks of age with septic shock and severe respiratory failure, the “control” non-genetic version stated that the genetics test was normal. The baby needed a central catheter inserted for antibiotics. I would hope that, if that happened in real life, the neonatologist, if unaware of the real implications of William’s syndrome, would consult colleagues and discover that William’s syndrome is a condition with variable and relatively mild intellectual impairments and a range of other moderately serious medical problems. I would not have thought that many people would consider William’s syndrome an indication for limitation of care, but the responses to this case were similar to the first, and the graphic is almost identical, substantially more neonatologists would recommend palliative care if the genetic abnormality was diagnosed, than those who had the case scenario with a normal genetic test, and fewer would recommend having a central line inserted for the antibiotics. I find it disturbing, that a diagnosis of Williams syndrome, even in an extremely sick baby, would lead to a recommendation to not even insert a central catheter for antibiotics.
Genetics is a discipline that has advanced enormously since I was trained, and the advances seem currently to be exponential. It is not surprising that there is limited knowledge among neonatologists of what the implications of certain findings might be. It is incumbent on us to seek out those who really are knowledgeable if we get back a genetic test result that we are uncertain about, and certainly not make life or death decisions that are not rational, and are based on misunderstandings.






