
Even the New England Journal are getting in on the act (Lee CD, et al. Neonatal Resuscitation in 22-Week Pregnancies. N Engl J Med. 2022;386(4):391-3), I guess that someone talked to the editors about the practice variation in resuscitation of profoundly immature babies, and in response they have published this short vignette with 2 somewhat opposing views, Leif Nelin who promotes the idea that we should recommend universal active intervention, and Elizabeth Foglia who is in favour of recommending selective resuscitation.
I find it very interesting that there is not a 3rd author promoting an approach which still happens in many centres, i.e. recommending universal comfort care.
It is also interesting that there is no real disagreement on the facts, that without active intensive care mortality is 100%; that with intensive care some babies survive, and the majority of the survivors have good lives. The actual proportion of survivors is, of course, very variable, and it requires a commitment of both obstetrics and neonatology to work together to achieve the best results.
Dr Foglia says 2 things that require some reflection, she notes that “almost all extremely preterm infants require resuscitative interventions after birth to survive” which is sort of true, but depends on what you mean by “resuscitative interventions”, in most centres all such babies have endotracheal intubation shortly after birth, but further “resuscitative interventions” are uncommon. The second thing is “The current limit of viability is 22 weeks’ gestation.” That is stated as a verity, but it ignores 3 things, 1. we never know exactly what the GA is, except after IVF, so if you actively intervene for all 22 week GA babies, you will have intervened for some at 21 weeks. 2. If survival at 23 weeks can be as high as 60%, surely at 21 weeks and 6 days it would not suddenly drop to zero! 3. There are reported survivors who were thought to be <22 weeks.
Current guidelines do not often recommend antenatal steroids at 22 and 23 weeks, which is partly because of a lack of such infants in randomized controlled trials, but we are unlikely to have substantial numbers of mother in trials at those gestations for a while, if ever, so observational data are all we are likely to have. Rossi RM, et al. Association of Antenatal Corticosteroid Exposure and Infant Survival at 22 and 23 Weeks. Am J Perinatol. 2021(EFirst). This article, as one example, calculated the probability of survival at 22 and 23 weeks of GA, according to whether steroids were given prior to delivery. The data source they used had no information of timing of steroids, it was just a checkbox, yes or no. It probably includes, therefore, many babies with brief steroid exposure. Survival is only presented for babies who received active neonatal intensive care. The overall survival at 22 weeks, to one year of age, is shown below, divided by birth weight categories.
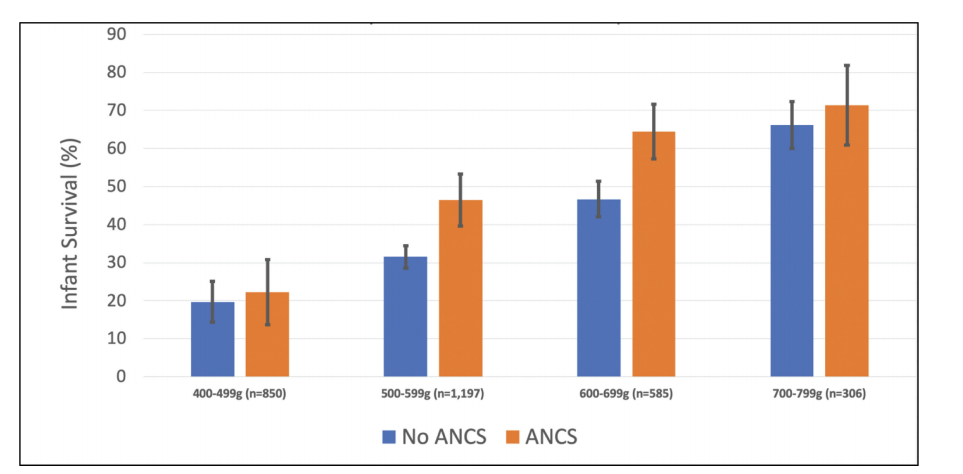
They don’t have the same sort of birth weight breakdown for the 23 week babies, but overall 1 year survival was 58% after antenatal steroids, and 48% without steroids. Relative risk 1.5 (95% compatibility intervals, 1.3-1.6). 62% of the 22 week deaths of babies who had antenatal steroids were before 7 days of age, as were 53% of the 23 weeks infants.
Currently all the data about such deliveries is consistent, ANS administration is associated with a major improvement in survival, the NNT is actually smaller than at any later GA. All the studies, unfortunately, suffer also from the same biases, which are sort of self-evident.
What is also consistent, is that centres with the best results, have a co-ordinated approach with obstetrics, and routinely give steroids as soon as the mothers are admitted.
As for my response to the NEJM article? I would perhaps phrase it a little differently, I think that active neonatal intensive care should be offered as an option to all mothers presenting with an increased risk of delivering at 22 to 24 weeks gestation, and that option should be presented as a reasonable choice which will be supported by the whole team, who will then do whatever they can to have the best possible outcome. When additional risk factors are present, such as growth restriction, imminent delivery without benefit of significant ANS exposure, then the discussion of the options must recognize those facts. When increased risk is very great, such as estimated weight <400g or florid chorioamnionitis, then it is vitally important to be realistic. It is also important to recognize that the decision to give steroids, as soon as possible, does not mandate active neonatal care, but will give the best chance for the baby if the later decision is indeed to proceed with intensive care. And that a decision for such care does not mandate a cesarean delivery, which should be considered a separate (obviously related) decision, which takes into account additional factors, including maternal age, risk factors etc.







Hi Keith,
You might be interested in our new publication reporting rates of active care and infant survival rates in Victoria in 2009-2017 in a whole-of -state population of babies born at 22-24 weeks’ gestation. We found lower rates of ANC exposure in babies not offered active care (as you would expect) and higher rates in those for whom active care had been provided. That was seen in babies born at 22, 23 and 24 weeks’ gestation.
Boland, RA., et al. (2021). Temporal changes in rates of active management and infant survival following live birth at 22–24 weeks’ gestation in Victoria. ANZJOG, doi:https://doi.org/10.1111/ajo.13309.
But we also found that many clinicians providing care and parent counselling did not have accurate perceptions of outcome of the babies born at 22-25 weeks- underestimating survival and overestimating rates of major disability. And, that clinicians were less accurate in their estimations of outcome in 2020 than they were a decade ago in 2010.
Boland, RA., et al. (2021). Disparities between perceived and true outcomes of infants born at 23–25 weeks’ gestation. ANZJOG Online First), 1-8. doi:https://doi.org/10.1111/ajo.13443
So the questions we pose are: What are we telling the parents about their infant’s potential for a good outcome? And how do misconceptions about outcome affect parent counselling and decision-making in babies born at 22 and 23 weeks?
More research needed to explore this!
Dr Rose Boland
Melbourne, Victoria
Thank you Keith. I think we have to remind ourselves that it is not our baby or the hospital’s baby. We must inform the parent’s of what might happen and then their desires and opinions should be followed. If they want the baby to have “a fair go” as the Aussies would say that should be respected. Even if the baby only survives a few hours, or days, they can feel they have tried and done their best. As obstetricians and neonatologists we should be prepared to give the baby the best treatment we know and not be half hearted about it. After all, it is the parents who will have the responsibility and hard work of caring for the child. The era of paternalistic doctors making all the decisions should now be behind us.