
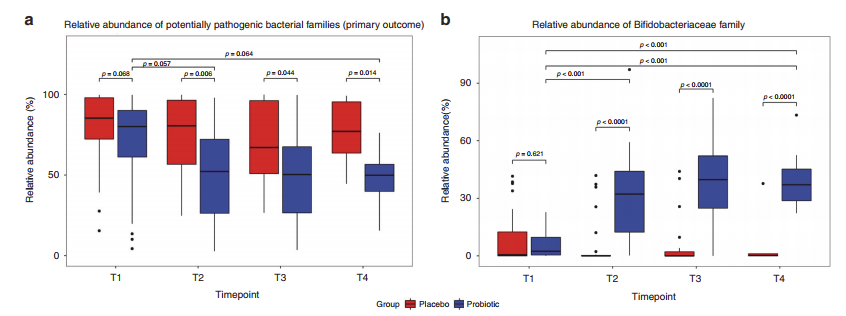
Rao S, et al. Probiotic supplementation in neonates with congenital gastrointestinal surgical conditions: a pilot randomised controlled trial. Pediatr Res. 2022. When we started using probiotics there had been a couple of case reports of probiotic associated sepsis in infants with congenital GI anomalies, specifically omphalocoele, so we decided to not include them in our probiotic protocol. I was never too sure that was the right thing to do, especially as infants with gastroschisis in particular are at high risk of NEC. The group from Perth, Western Australia, randomized 61 babies to a Bifidobacterium mixture (B. breve, B. longum longum, and B longum infantis) or placebo and followed their intestinal microbiome development weekly until discharge, they found that there was a progressive change in the microbiome due to supplementation, with less dysbiosis, specifically a lower abundance of potential pathogens (Clostridiaceae, Enterobacteriaceae, Enterococcaceae, Pseudomonadaceae, Staphylococcaceae, Streptococcaceae &Yersineaceae) and much more Bifidobacteria. In a pilot study of this size one wouldn’t necessarily expect to see a clinical impact, although growth parameters were improved with probiotics, in particular head growth; or rather, the postnatal growth restriction, was less severe in the probiotic growth.
Plummer EL, et al. The effect of probiotic supplementation on the gut microbiota of preterm infants. J Med Microbiol. 2021;70(8). This study analysed the intestinal microbiomes of infants randomized in the ProPrems trial, which was a large multicentre trial of a mixture of B longum infantis, B animalis lactis and Streptococcus thermophilus vs placebo. 99% of the babies in the probiotic group had the Bifidobacterial DNA in their stools during treatment, but in only about 90% of the fecal samples, about 20% to 35% of the controls also had the bacteria in their stools at times. The relative abundance of the B infantis was quite variable, suggesting we need to find ways to make colonization more effective.
Hui Y, et al. The effect of early probiotic exposure on the preterm infant gut microbiome development. Gut Microbes. 2021;13(1):1951113. This is a study of microbiome development in 2 cohorts of preterms, before and after routine probiotic use (a mixture of Lacticaseibacillus rhamnosus GG, the bacterium formerly known as Prince Lactobacillus, and Bifidobacterium animalis ssp. lactis) in Copenhagen. They showed less impact on the progression of microbiome changes than some other studies, associated with a variable abundance of the probiotic organisms, but did show an impact leading to a reduction in Klebsiella concentrations in the stools.
Fleming P, et al. Bifidobacterium breve BBG-001 and intestinal barrier function in preterm babies: Exploratory Studies from the PiPS Trial. Pediatr Res. 2021;89(7):1818-24. This is an analysis of microbiome impacts and intestinal functional impacts of the B breve used in the PiPs trial. In addition to the usual 16sRNA, they also cultured the stools, and found they were able to grow Bifidobacteria, identified by pcr as B. breve, from most of the probiotic babies, as well as some controls, but found that babies colonised with B breve actually had more potentially pathogenic Enterobacteriacae from 3 weeks onwards. They did not see a benefit on intestinal barrier function of the probiotic.
Overall, I think these recent studies imply that the best probiotic to have an impact on the preterm infant microbiome, and, as a result on NEC, is Bifidobacterium Longum subsp. Infantis. Other data from network meta-analysis that I have discussed previously, is also consistent with this, and also consistent with a benefit of a mixture of Bifidobacteria (most mixtures include B infantis). Ways of ensuring good colonisation, such as the addition of prebiotics, especially Human Milk Oligosaccharides, and provision of human milk will probably help to ensure the greatest benefit.







Thank you Keith. Recommending and or using probiotics for preterm babies is a very interesting area but needs to one considered with some circumspection. Does the product actually contain the bacteria stated on the label and does it have them in the number stated? Are there enough to have an effect? Are the bacteria are able to survive long enough to reach your gut without being digested by the stomach? If they do survive too be passed in the stools are they being passed to control babies in the NICU? For a clinical trial have the bacteria, and numbers been independently verified? There is little evidence for the dose “number” which are most effective. Some can be bought over the counter and may not be produced to the standard required. There are many different types of probiotics and different combinations that may have different effects on the body, and little is known about which are best. Recommendations for their use in the clinic or in research studies need to be species and strain specific. Lastly, they are said to be “friendly bacteria” but in neonatal medicine we may be giving them to very immature, immunocompromised babies. There are cases of infection in immunocompromised adults. I don’t know if they are detected in routine blood cultures done on perm babies.
You are of course right that we should not go to our local health food store to pick up a probiotic mix. Many such preparations contain no live organisms, and when they do they are often not what is advertised on the label, and some of them contain pathogens. A preparation with optimal quality control and clearly defined contents is essential. That being said, such preparations are available, in Canada, the UK and the USA, and across Europe.
It is possible to have sepsis with the organisms; before we started using them we ensured that our lab could grow the bugs in “Flora-baby”, which they could, even though precise identification is difficult. We have had 3 babies with positive bifidobacterial cultures, finally identified by our regional lab as being species that are in our preparation. They were mildly ill, and easily treated and all survived. Other publications of bifido and lactobacillus sepsis have similar findings. Overall late-onset sepsis is less frequent with probiotic prophylaxis, and the risk benefit is clearly in favour of probiotic prophylaxis, if you can find an appropriate preparation.
ThAnk you. The Taiwanese were some of the first to publish about this. I went to meet them. They ask the parents to go to a pharmacy and buy some. Hopefully now that is better.
I am not convinced that probiotics are more efficacious than mother’s milk.