
My previous post about the FETO trials noted that the published trials reported a clear benefit of antenatal treatment of the highest risk group, but the moderate risk group had an improved outcome which didn’t meet classic definitions of statistical significance. I noted then that, if the trials had been run as a single trial with 2 risk strata, the overall benefit for the entire sample would have been highly significant, and that it was likely that a test for interaction would not have shown a statistically significant difference between the risk strata.
That evaluation has been confirmed by an analysis published by the authors, (Van Calster B, et al. The randomized TOTAL-trials on fetal surgery for congenital diaphragmatic hernia: re-analysis using pooled data. Am J Obstet Gynecol. 2021), they pooled the data from the trials and found no significant difference in the benefit of FETO according to risk category. The surgical protocol for the trials included intervention and FETO at 27 to 29 weeks and 6 days in the severe group, or 30 to 31 weeks 6 days in the moderate group.
In this re-analysis the authors looked at the GA of intervention and conclude that FETO leads to improved survival in both the severe and the moderate groups, indeed overall there was no impact of severity (O:E LHR) on effectiveness of the procedure, rather it seemed that earlier treatment was associated with greater improvements in survival, but also greater increases in prematurity.
These 2 figures show the survival advantage of having FETO as compared to usual treatment based on the O:E LHR, even with the lowest risk babies in the trial, FETO is advantageous, as shown by the blue line and the blue shaded area representing the confidence limits of the benefit. The dotted lines are what the predicted survival benefits would have been if the babies had FETO at different GA, not allowed by the protocol, suggesting an even greater survival benefit for the moderate babies if they had FETO earlier.
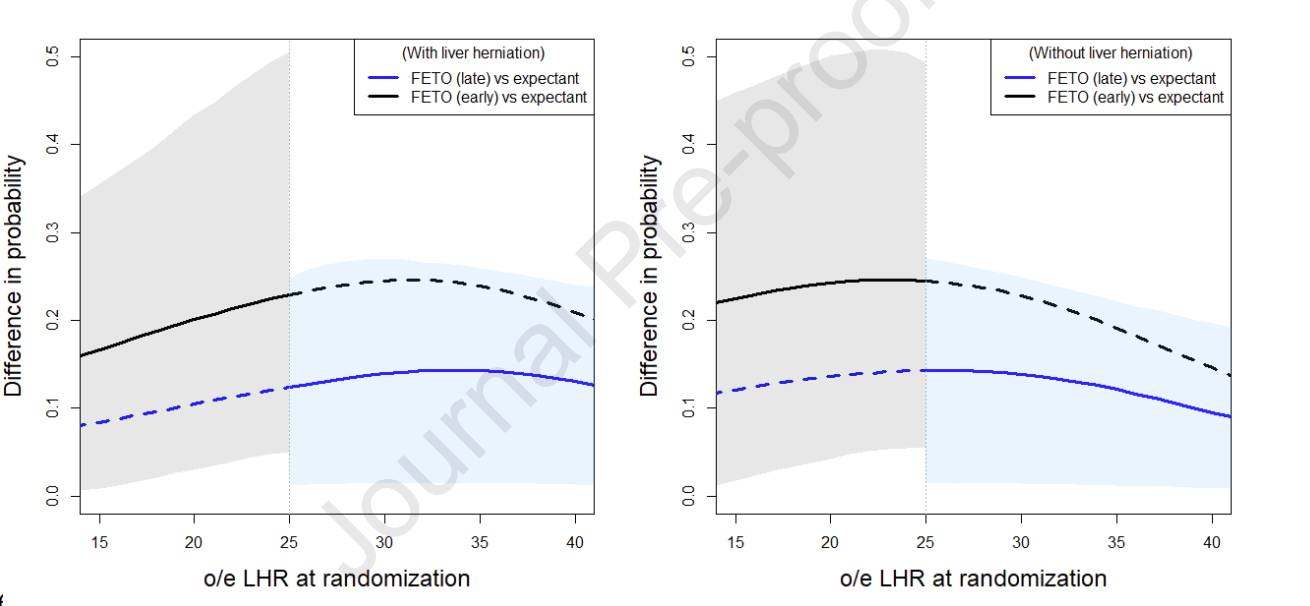
Of course this analysis is confounded by the correlation between severity and timing of intervention, as by design more severe lesions were treated earlier.
The next challenge will be to find ways of preventing membrane rupture and preterm labour after fetoscopic intervention, if we can do that, then the benefit of FETO for improving survival will likely be even greater. I think this analysis confirms, that, if it is available, FETO should be discussed with mothers carrying fetuses at moderate risk, not just the most severely affected.






