
I am still unconvinced that transfusion associated NEC is a real thing, I think it is possibly a real phenomenon, but I am not sure how to know for sure.
Some of the best evidence I think comes from the PINT trial, a randomized trial of transfusion thresholds. The preterm infants in the high threshold group received many more transfusions, but did not have more NEC, in fact they had less NEC 5.3% vs 8.5% (RR with restrictive transfusion 1.62 (95% CI 0.8, 3.26). The other 2 RCTs included in the Cochrane systematic review that reported NEC were much smaller and did not contribute much to the meta-analysis which thus gives the same overall RR of 1.62).
In the RCTs of later use of erythropoietin, babies in control groups had many more transfusions, but the Cochrane systematic review does not show a major difference in NEC, RR 0.88 with epo, (95% CI 0.45, 1.7).
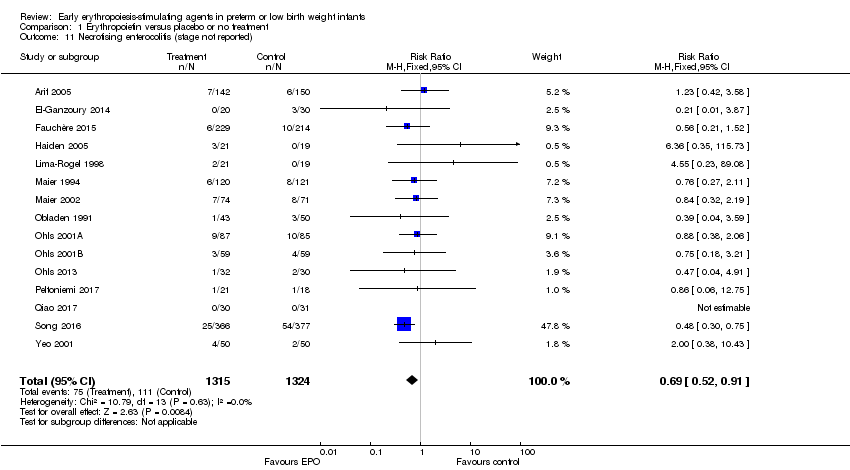
In contrast, the Cochrane systematic review of early use of erythropoietin does show less NEC with epo, and, of course, the epo babies also had fewer transfusions.
An observational study from 2016 might explain some of the confusion, They suggest that severe anemia might be associated with NEC, rather than red cell transfusion. (Patel RM, et al. Association of Red Blood Cell Transfusion, Anemia, and Necrotizing Enterocolitis in Very Low-Birth-Weight Infants. JAMA. 2016;315(9):889-97). They used the data from a prospective cohort study of transfusion related CMV in preterm infants; because of variations in practice, as indications for transfusions were not standard, they could attempt to analyze the separate impacts of transfusion and anemia, with a hemoglobin less than 80g/100mL. They included 600 VLBW infants, who had 42 episodes of at least stage 2 NEC. About half of the babies were transfused, and they were smaller, less mature and sicker than non-transfused infants, and 18% had at least one hemoglobin under 80.
The rate of NEC was increased in VLBW infants who received RBC transfusions compared with infants who did not (cause-specific HR, 2.33 [95% CI, 1.18-4.60]; P = .01)….
In multivariable analysis, including adjustment for birth weight, duration of breastfeeding, illness severity, severity of anemia, duration of antibiotic treatment, and center, any RBC transfusion in a given week was not independently associated with an increased rate of NEC (cause-specific HR, 0.44 [95% CI, 0.17-1.12]; P = .09) or mortality (cause-specific HR, 1.36 [95% CI, 0.27-6.82]; P = .71)…. In a given week, VLBW infants with severe anemia had a higher estimated rate of NEC compared with VLBW infants without severe anemia (adjusted cause-specific HR, 5.99 [95% CI, 2.00-18.0]; P = .001).
Of course because transfusion is used to treat anemia, and babies with more severe anemia are more likely to be transfused, these are things that are difficult to separate, but these data do at least suggest that it is severe anemia, rather than transfusion which increases NEC.
I think this all might add together, with early epo there is less severe anemia, and thus, if the association is actually causative, there should be somewhat less NEC; in the PINT trial the high transfusion threshold group were unlikely to develop severe anemia, and so were less likely to develop NEC. In normal clinical practice we are more likely to transfuse the most anemic babies, and thus there is an apparent association between transfusion and NEC. Confirmation of this from another database, and analysis of the TOP trial when completed (I think enrolment has finished and outcome assessment should finish this year) will be important to answer these questions.
The study that I am blogging about is fairly old news, for my blog, from 2016, but I was reminded of it as we have been working on developing standardized transfusion criteria, and by a couple of recent publications:
Does severe anemia really affect the gut? A prospective study from Turkey measured fatty acid binding proteins in very anemic babies before and after transfusion (Ozcan B, et al. Severe Anemia Is Associated with Intestinal Injury in Preterm Neonates. American journal of perinatology. 2019). Intestinal FABP and liver FABP are apparently good markers of intestinal injury, and previously liver FABP has been shown to increase with NEC of all grades, and I-FABP only with very severe NEC. In this new study I-FABP was only slightly higher among anaemic babies than among controls, but liver-FABP was appreciably higher, and remained high 48 hours after transfusion.
Another relevant recent publication is from a mouse model (Arthur CM, et al. Anemia induces gut inflammation and injury in an animal model of preterm infants. Transfusion. 2019;59(4):1233-45). In this study they correlated cytokine concentrations in preterm infants with their hemoglobin levels, more anemic samples had higher Interferon alpha levels. They then performed a mouse study gradually bleeding the mice to anemia (PIA ia phlebotomy-induced anemia) and performing a number of fascinating analyses of their intestines.
Gradual induction of PIA in a pre‐clinical model resulted in significant hypoxia throughout the intestinal mucosa, including areas where intestinal macrophages reside. PIA‐induced hypoxia significantly increased macrophage pro‐inflammatory cytokine levels, while reducing tight junction protein ZO‐1 expression and increasing intestinal barrier permeability.
Preventing severe anemia with a combined approach of delayed cord clamping and erythropoietin should lead to less NEC if these findings are real; a systematic review of delayed cord clamping did show a bit less NEC RR=0.88 [95% CI 0.65–1.18], although they marked the quality of this evidence as low. (Fogarty M, et al. Delayed Versus Early Umbilical Cord Clamping for Preterm Infants: A Systematic Review and Meta-Analysis. Am J Obstet Gynecol. 2017), I am not sure how effective delayed clamping is in preventing late severe anemia, I don’t think that has been reported often in the studies, but early hemoglobin is, of course, higher. But a few weeks later, after being in the ICU for a while, with multiple blood sampling and intercurrent illnesses, the effects of delayed clamping on late severe anemia might well be dissipated. On-going trials of erythropoietin for brain-protection in preterm infants may also be able to answer questions about anemia and NEC, depending on doses and duration.
Thinking about it, I am not sure why many of us went of the routine use of erythropoietin, I guess we were all focused on trying to reduce donor exposure, which is generally unaffected with current transfusion practices. I think avoiding blood transfusions and reducing severe anemia are probably valuable goals in themselves. Maybe we should rethink erythropoietin/darbepoietin routine use.







And does feeding during a transfusion play a role? Mixed results here. My own recollection over decades of practice is that therr had been more transfusion associated NEC following transfusion for profound anemia.
It’s of course possible that severe anemia makes the gut more at-risk for re-oxygenation injury with a transfusion.