
When do you give a platelet transfusion? You could easily ask 10 different neonatologists and get 15 different answers. I would be one of those who gave several different answers depending on the clinical situation, believing that thrombocytopenia of different aetiologies probably should be transfused at different thresholds, but not knowing the right threshold for any condition. I thought that platelet transfusions were pretty safe, however, so if a colleague transfused at 50,000 a baby that I would have let fall to 30,000, it didn’t bother me very much.
Questionnaire studies have highlighted the differences in transfusion approaches and practices have been analyzed in studies such as this one, in which 1/3 of transfusions were given to babies with a count over 50,000 (per cubic millimeter, I won’t repeat the units after this). There was never, however an appropriate evidence base to decide on thresholds.
To answer the question I think you should, first of all, study separately the babies with early thrombocytopenia due to alloimmunization, and the few due to maternal auto-immune thrombocytopenia. Maybe you should also eliminate those with thrombocytopenia associated with placental failure/IUGR, and then randomize the remaining babies, many of whom would have sepsis, or NEC, or CMV, to receive platelets at different thresholds, and see if the higher threshold reduces bleeding compared to a lower one. I would probably leave out the IUGR babies as they almost never seem to bleed, but that may not be true, and we certainly need to know.
That is just about exactly what was done in the just-published PLaNeT-2 trial, which just appeared on-line at the formerly prestigious NEJM. Curley A, et al. Randomized Trial of Platelet-Transfusion Thresholds in Neonates. New England Journal of Medicine. 2018.
This trial enrolled babies of less than 34 weeks gestation and included babies with IUGR: (the protocol has previously been published (Curley A, et al. Platelets for Neonatal Transfusion – Study 2: A Randomised Controlled Trial to Compare Two Different Platelet Count Thresholds for Prophylactic Platelet Transfusion to Preterm Neonates. Neonatology. 2014;106(2):102-6) and the whole protocol is available as a supplementary file on the NEJM.org).
Babies with a platelet count of less than 50,000 who had a head ultrasound less than 6 hours previously were randomized. I guess they did this by screening babies with a platelet count of less than 100,000, and performing a head ultrasound if they thought they would become eligible. Babies who had a hemorrhage within the previous 3 days were not eligible.
The primary outcome variable was survival to 28 days (after randomization) without a major hemorrhage : “The outcome of “major bleeding” included intracranial hemorrhage (leading to neurosurgical intervention or radiologic imaging showing midline shift), intraventricular hemorrhage filling 50% or more of the cerebral ventricle, pulmonary hemorrhage (fresh bleeding through an endotracheal tube with increased ventilatory requirements), frank rectal bleeding, and severe bleeding (fatal bleeding, life-threatening bleeding associated with shock, or bleeding requiring fluid boluses or red-cell transfusion). Our definition of rectal bleeding was pragmatic; we defined any amount of fresh visible blood as rectal bleeding”.
660 babies were enrolled in 43 trial sites in the UK, Ireland, and Holland. When transfused babies received 15 mL/kg of platelets. Study size was determined from an expected 20% incidence of major bleeds in the low threshold group, and a desire to detect a reduction to 12% with a higher threshold
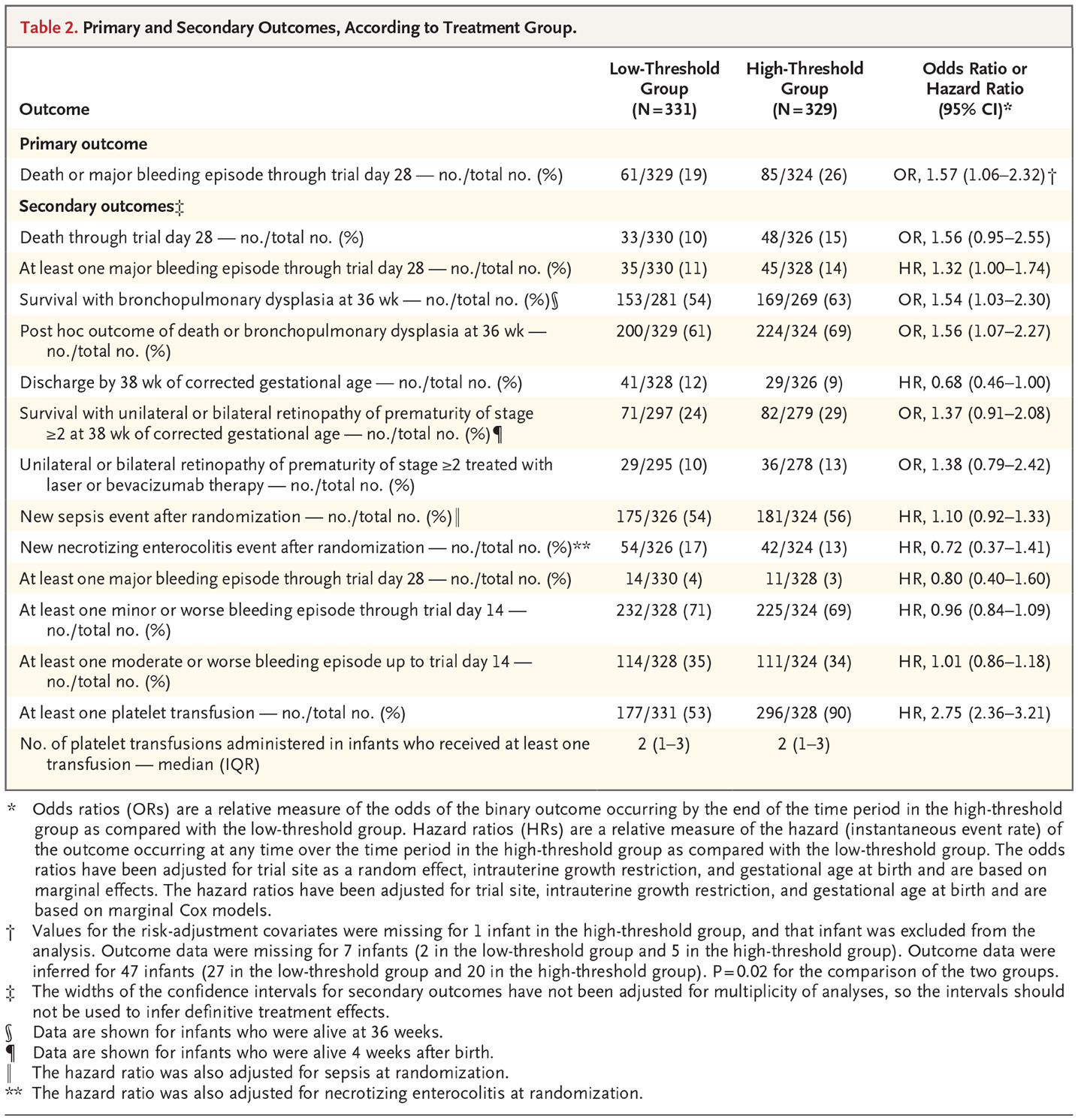
The 329 babies in the 25,000 threshold group had 61 major bleeds or deaths prior to 28 days, similar to the hypothesized rate at 19%, and the 324 babies in the high transfusion group had 85 bleeds or deaths which is 26%, for an Odds Ratio of 1.57 (95% confidence intervals 1.06, 2.32).
As you can see from the table with the maine results below, the difference was mostly in survival, although there were a few fewer bleeds in the 25,000 threshold group.

Most of the babies were several days old when enrolled, and many were septic or had NEC. There is really no evidence at all of any benefit of transfusing at a higher threshold from these numbers.
I can’t find in the publication or supplemental data the numbers of babies who survived to discharge, which is much more relevant to me than survival to 28 days after enrolment, if the differences disappear over the subsequent few weeks to discharge (the babies were on average 26 and a half weeks gestation, and about 750 g birth weight so they would have been around for several weeks after the trial) then the implications might be different.
Despite that, I think the lack of any apparent benefit, and possible harm, from transfusing more liberally, and given that this is the only prospective reliable data on outcomes of different platelet transfusion thresholds in the premature, babies at risk of bleeding from thrombocytopenia should be left to fall to 25,000 unless they are actively bleeding. Or maybe even lower.







Pingback: Platelet transfusion threshholds: 25,000 even for the highest risk infants? | Neonatal Research