
Neonatology ‘grew up’ treating babies with surfactant deficiency. We all learnt about recruiting lungs with PEEP, and that increasing mean airway pressure improved oxygenation.
It is generally true that babies with acute pulmonary disease of low-volume such as HMD, pneumonia, and some babies with meconium aspiration, increasing mean airway pressure improves oxygenation. I remember an old paper from my mentor Neil Finer, that showed that all ways of increasing MAP were not equivalent. For the same increase in mean airway pressure, increasing PEEP was more effective, in terms of increasing oxygenation, than increasing the peak inspiratory pressure or changing the Inspiration:Expiration ratio. Increasing lung recruitment by maintaining a higher pressure in the lungs during expiration, thus improving end-expiratory lung volume, improves V/Q matching.
Unfortunately this has led to the tendency to always increase PEEP, and/or mean airway pressure, when oxygenation is a problem.
But some lungs are not recruited by increasing PEEP. Specifically, babies with pulmonary hypoplasia do not benefit from increased PEEP, (unless they also have HMD).
In contrast, increasing PEEP in such babies has a number of potential adverse effects. These have been very nicely demonstrated by a recent article reporting a cross-over study in 17 patients with congenital diaphragmatic hernia (CDH) and pulmonary hypertension. (Lower Distending Pressure Improves Respiratory Mechanics in Congenital Diaphragmatic Hernia Complicated by Persistent Pulmonary Hypertension, Guevorkian D et, J Pediat 2018) In the postoperative period infants were randomly placed on a PEEP of 2 or 5 cmH2O for an hour, and then switched to the other pressure. Lung mechanics and hemodynamics were measured at the end of each hour. The peak pressure was adjusted by 3 cmH2O also, in order to keep the ‘delta-P’ unchanged.
Lower PEEP led to substantially higher compliance, higher tidal volume, and much lower PCO2. Left pulmonary artery blood flow velocities, diastolic left ventricle diameter, and the left atrium to aorta diameter ratio were greater at 2 cmH2O of PEEP compared with 5 cmH2O. Here is the compliance figure:
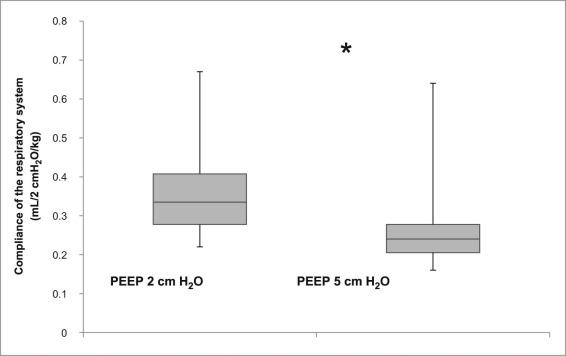
Of note, at 2 cmH2O oxygenation was much better, oxygen requirement dropped from 35% at a PEEP of 5 cmH2O, to 25% at 2 cmH2O, with a preductal saturation that was higher, and a post-ductal saturation that was much higher at the lower PEEP (Mean 91% compared to 81%).
In other words, increasing PEEP from 2 to 5 cmH2O led to overdistension of the lungs, pushing them to a higher, flatter part of the pressure volume curves (decreasing compliance and minute ventilation), and led to compression of the pulmonary vasculature which increased shunting, and worsened ventilation and oxygenation.
There is little previous data to compare this to, but a study in 2000 from Dresden measured FRC directly in 5 patients with CDH both before surgery and after, and also measured lung mechanics. They used varying PEEP levels, between 1 and 4 cmH2O, for the postop measurements. They showed that after surgery, at a PEEP of 4, there was a reduction in compliance compared to pre-op, and that with reductions in PEEP to 1 cmH2O compliance progressively improved, FRC was about 20% higher at a PEEP of 4 than at 1 cmH2O, confirming the obvious interpretation that the adverse effects of PEEP were caused by an increase in lung volume, and overdistension. They also studied the effects of suction on the chest tube, and showed similar effects, with increasing FRC and decreasing lung compliance as suction increased from 0 to -10 cmH2O.

Although both of these studies show the effect in the postoperative period, I can’t see any good reason that the effects would be different pre-operatively, or indeed in other patients with pulmonary hypoplasia.
You can see similar effects in babies with HMD who have had a good response to surfactant. There are a few articles that have measured mechanics and lung volumes at different levels of PEEP after surfactant treatment. They show that over-distension of the lungs at relatively low levels of PEEP is frequent, Eduardo Bancalari’s group compared PEEP of 2, 4 and 6 cmH2O, Anne Greenough studied 0, 3 and 6 cmH2O, Dinger et al from Dresden compared 0.2, 0.3 and 0.4 kPa (which is almost exactly 2, 3, and 4 cmH2O, I believe) . All the studies in preterm babies after surfactant show, as you would expect, that if you use higher pressure during expiration the lung volume will be higher, they usually also show a decrease in compliance as the PEEP increases.
These findings explain a paradox that often baffles fellows when they start neonatology. Dynamic respiratory compliance, in several studies, does not improve after surfactant therapy if you leave the ventilator settings unchanged. FRC increases substantially however, and if you reduce PEEP after the surfactant, then you will see an improvement in compliance, this is evident with volume guarantee ventilation, peak pressures don’t change after surfactant until you drop the PEEP a little, then you will see much greater decreases in the peak inspiratory pressure than the change you made to the PEEP.
Overdistension of lungs in babies with diaphragmatic hernia is common and easy to achieve even with relatively modest levels of PEEP.
In preterm babies, after surfactant, also.
Once the fetal lung fluid has been resorbed in the first few minutes of life, most babies with CDH should be managed with very low PEEP. The same applies to babies after surfactant who fall to 21% oxygen or near to it, the most immature babies, and those with CDH have very fragile lungs and improving their outcomes requires that those lungs be protected.







My daughter is expecting a child in 4 weeks and was told that he has a very rare case of a neuroenteric cyst in his diaphragm. How likely is this to ability to breath on his own? How is this condition likely to manifest itself? What are the concerns associated with this problem?
Hi, honestly this is so rare that I couldn’t give you much information. The few cases that have ever been reported have variable presentations, some can be very sick with difficulty in lung function, others are relatively minor. As a general rule (and I can’t give individual advice) such a baby should be delivered in a centre with experienced pediatric surgeons, and all the support services available, what we would call a level 4 or sometimes a level 3b centre. I don’t remember ever seeing a case myself, even though I work in just such a centre! Hope all goes well.
Thank you so much for your response. Does the size of the cyst have any significance in this situation? I believe that it is extremely small. Perhaps it is the location that is more important? How much does birth weight play a role? He is now in the lower 25 percentile. I appreciate your help.