
Towards the end of last year the Canadian Pediatric Society published a new ‘position statement’. These are official proclamations of the society, supposedly based on the best available evidence to guide practice, and which become de facto standards of care. This particular one ‘Counselling and management for anticipated extremely preterm birth’ presented an opportunity to update a 20 year old statement.
Unfortunately it is a failure. It promotes an unethical standard based on simplistic thresholds of intervention. I have been writing a response to this for a while, and following the commentary in the CMAJ by Dan and Beau Batton, which makes many of the same points, I thought I would share this, in various different sections; this is the first.
This series of posts are a very expanded version of a commentary that has been accepted for publication in ‘Paediatrics and Child Health’. That commentary was written by a large group of collaborators from around the world, but is only 1500 words long, to comply with the word limits. I have taken the ideas from that commentary and developed them here.
The CPS position statement makes the following recommendations:
- At 22 weeks’ GA, since survival is uncommon, a non-interventional approach is recommended with focus on comfort care. (Strong Recommendation)
- At 23, 24 or 25 weeks’ GA, counselling about outcomes and decision making around whether to institute active treatment should be individualized for each infant and family. (Strong Recommendation)
- At 23 and 24 weeks’ GA, active treatment is appropriate for some infants. (Weak Recommendation)
- Most infants of 25 weeks’ GA have improved survival and neurodevelopmental outcomes and active treatment is appropriate for these infants except when there are significant additional risk factors. (Weak Recommendation)
I will leave aside for the moment the ‘strong’ and ‘weak’ recommendation part of this, more on that later, (see part 2).
This post will address the first 4 of the many failings in these recommendations;
1. Gestational age is only known imprecisely.
2. there is no explanation on how these thresholds were picked,
3. gestational age is only one part of risk assessment for these babies, and
4. the values and wishes of the parents are not mentioned.
1. Firstly, we never know the gestational age, except after in vitro fertilization. Recommending precise thresholds for intervention based on a number that is very imprecise is ridiculous. At its best, ultrasound, performed at around 12 weeks, can be plus or minus 5 days, 95% of the time. How can you recommend changing from one recommendation to another at a precise day, when the true gestational age may be 5 days more or less? Surely we need to recognize this limitation, and counsel families according to a range of possibilities based on GA plus or minus 5 days, as well as on other factors which affect survival. If the ultrasound is performed between 14 and 18 weeks the accuracy is plus or minus 10 days, after 18 weeks ultrasound is completely unreliable for assignment of GA.
2. Nowhere in the discussion preceding the recommendations is there any rationale given for not intervening at 22 weeks, but considering intervention at 23 weeks. In other words, why not start considering intervention at 23 weeks and 3 days? Or why not at 24 weeks, 2 days and 17 hours? Surely it couldn’t be just because it is a nice round number? This position statement, and others like it, can be lethal. Making potentially lethal statements which are based on a nice round number that happens to coincide with our traditional division of time into 7-day periods is worse than irrational. What changes at 23 weeks, 0 days and 0 hours to make intervention optional, when it was not even an option previously? This is never explained.
When you combine these 2 problems, the situation become ever more ridiculous, a mother in threatened preterm labour who presents with a best-guess gestational age of 23 weeks and 4 days, if you have a good quality 10 weeks dating ultrasound, has a 95% lower probability limit of actually being 22 weeks and 6 days, and therefore supposedly not eligible for active intervention. The 95% upper probability limit of gestational age would be 24 weeks and 2 days, which according to this statement changes everything.
But it is the same mother, the same family, the same fetus.
3. Survival of infants who receive intensive care at a best-guess gestational age between 22 weeks and 0 days and 22 weeks and 6 days (plus or minus 5 days!), when considered as a group, varies from 10% to 34% in different places who are willing to give active perinatal care, and, obviously, it is 0% if they are not willing to do so.
But we aren’t treating a group of babies, we are, potentially, treating individuals, some of whom have very poor chances of survival, and other who have chances of survival which are very much better. If you take the data from the NICHD network, the chances of survival at 22 weeks vary by more than 20-fold depending on other factors such as sex, birth weight, and having received steroids. The NICHD calculator gives chances of survival of between less than 1 % to more than 20% for individual babies born at a ‘best-guess GA’ of 22 weeks. We also know that infants whose ‘best-guess GA’ at birth is nearer to 23 weeks are more likely to survive than babies just at or just after 22 weeks. To lump them all together, just because it is easy, is doing a major dis-service to their families. For some babies, under certain circumstances, active intervention before 23 weeks gestation is a reasonable option, and if consistent with the families values and their wishes it should be considered.
A blanket recommendation to never intervene before 23 weeks gestation ignores all of these other factors. (gestational age uncertainty, other good or adverse risk factors, parent’s values, extra days of gestation…)
At the other end of this period of gestation, the statement reads ‘Most infants of 25 weeks’ GA have improved survival and neurodevelopmental outcomes and active treatment is appropriate…’. (First of all this makes no grammatical sense, ‘Most have …improved’, what does that mean; compared to what?) But more importantly, some infants born at 25 weeks have very poor chances of survival, many others have excellent chances, a boy born at 25 weeks and 1 day (plus or minus 5 days) who is small for gestational age and hasn’t had a chance to get steroids has a much lower chance of survival than a baby of 25 weeks and 6 days (plus or minus 5 days) with higher than average birth weight who has had steroids. Lumping them together is senseless. Just as importantly the girl at 24 weeks and 3 days (plus or minus 5 days) who has had steroids and has a good birthweight also has a much better chance of survival and a much better outcome than the previously mentioned SGA infant without steroids. But she is on the wrong side of this nonsensical divide, so her life is considered optional.
There is so much overlap between the outcomes of infants born at ’24 weeks’ and those born at ’25 weeks’ that it is unhelpful to divide the infants up this way.
Counseling a mother with threatened extremely preterm delivery should start with a risk assessment which must take into account her probable gestational age (with its inherent uncertainty) the estimated fetal weight (with its even greater inherent uncertainty, see below) the place of birth, whether the mother has been administered steroids, and whether the baby is single or if it is a multiple gestation, and then explore her values and the family’s desires.
The graph below illustrates how little sense it makes to base decision making on gestational age. They are data from a fairly new study from the Trent region of the UK Manktelow B and others, recently released in Pediatrics. 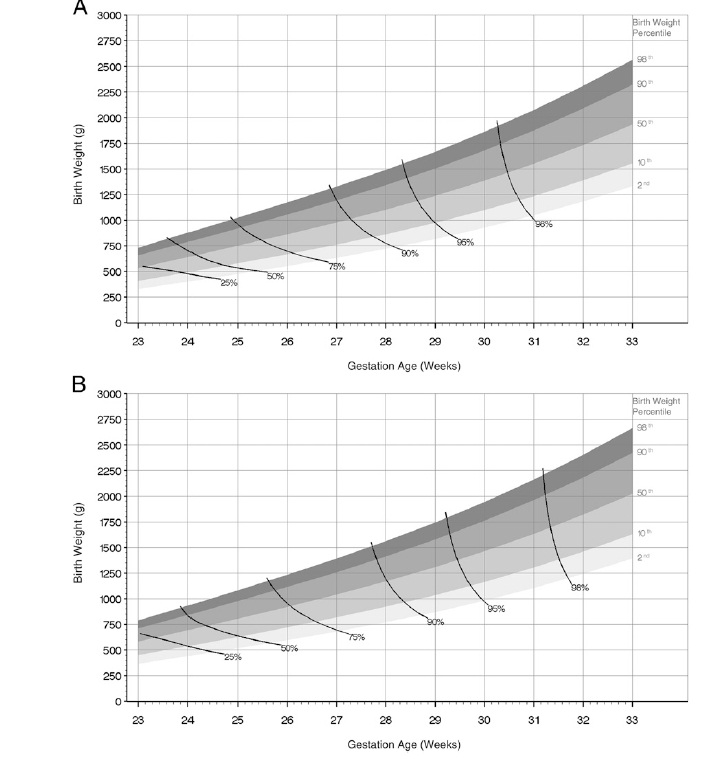
The top panel is for girls, the bottom one for boys. The graphs show the different weight percentiles at increasing gestational ages, and the solid lines join combinations of weight and gestational age which have the same mortality. If a GA based guideline made sense then these lines would have to be close to vertical, and be the same for boys and girls. In fact they are closer to horizontal, the graphs would have to be multi- dimensional to also include the effects of having had steroids and being multiple or a singleton, but those factors also affect survival. In fact the near horizontal line at very low gestations means that birth weight has a closer relationship with mortality than does gestational age. Of course we don’t know the birth weight before delivery and estimated fetal weights can be helpful, as a sort of general guide, but estimated weights are much more variable even than gestational age, being plus or minus 10%, 75% of the time (depending on the study you use to do the calculations).
These are complex and difficult decisions in moments of stress. Reducing them to a simplistic mantra based on completed weeks of gestational age is unethical.
4. Finally the recommendations must mention the values and desires of the parents, which, although discussed in the text, are not in the recommendations, surely they are pivotal. Surely they must be mentioned in the recommendations.
I think that externally imposed arbitrary limits for resuscitation are unethical. In any field of medicine. In this particular case, threatened preterm delivery, the uncertainties of gestational age assessment and the poor correlation of gestational age with outcomes makes this triply unethical.







Very well written. Thank you.
Canadian Premature Babies Foundation has written a letter to the Canadian Pediatric Society about their “new” position statement about “counselling and management of anticipated extremely preterm birth”.
As a family led organisation, we find the statement oversimplifies a situation that is highly complex medically, for families extremely stressful and often not anticipated.
Sorry for the length of it but I think it is worthwhile reading from a family perspective, so here it goes:
“Dear Board of the Canadian Pediatric Society
We read the Position Statement on “Counselling and Management for anticipated extremely preterm birth” and found that the statement could be enhanced by the family perspective. We would be happy to collaborate on a position statement that includes the views of families who have experienced premature birth. In our opinion, this perspective needs to be included in the Statement.
We would like to share some of our thoughts from a parental perspective on the CPS Position Statement.
Families with prematurely born children are thankful for the advanced medical care available in Canada and the support that the staff give them. We value the lives of our children, despite the challenges that might exist. They bring joy to those who love them. As a society we need to advocate for the most vulnerable.
This position statement is about decision-making for extremely preterm infants. Parents have to make very difficult and emotional decisions that are often not expected. Parents rely on the neonatologist to provide them with comprehensive and accurate information. Many parents want to consider “everything that can be done”, for their child because it is theirs and they want to share their lives with this baby. Parents often have differing views about death and disability than health care providers.
As families of preterm infants and as a foundation which exists to give them a voice, one of the first thoughts that came to our mind when we first read the CPS statement is that our children cannot be defined simply by gestational age. The length of gestation is not usually known to the exact day, except when conception occurs via in vitro fertilisation. Many factors influence the outcome of babies born very early. Were prenatal steroids given? What is the birth weight of the baby? Are the babies multiples? What is the gender of the baby? What pre-natal care was provided? These factors make a difference in how these children develop in their families.
The aim of the Statement is to make the “decision-making” process easier; but easier for whom, parents or doctors? It seems this Statement was written by physicians to simplify the prenatal consultation process for physicians. From a parental perspective, there are omissions in this Statement. The inclusion of a section on guidelines about communication with parents would be crucial. Discussions should be sensitive to the culture of the family. Communication should be personalized and in reference to each unique baby in the context of his/her own family, not simplified to a number of completed weeks of gestation. Prospective parents at risk of delivering preterm are all different. Some want a lot of information, some want general information, some want the long term prognosis, others want to know about the day to day life in the NICU. All parents need time and patience.
We disagree that all families need to receive extensive information, statistics and numbers about all the negative outcomes preterm infants may have. Families primarily decide with their heart. The decision that is taken for ones’ child has an impact on a family forever. Many of us had extensive ante-natal consultations where the neonatologist exposed us to a list of adverse events; many of these consultations were so negative and devoid of hope that we became very anxious and stressed. This is not healthy for the unborn child.
The decision-making section includes the sentence “some parents are reluctant to carry the burden of decision making, others want to be involved and have the expertise to do so, while yet others do not know how to be involved.” This sentence is somewhat bewildering. Who decides what expertise is needed to make life/death decisions? What kind of expertise is needed when you are talking about your own child?
The premature baby is viewed as generating high cost to our society by the authors. The statement does not once say what preterm babies and children can do, how they live happy lives and what they bring to their families and communities. The statement says that parent advocates were consulted. We would like to find out who they were. The statement is very negative. There are many reasons to have hope and at the very least, not take all hope away from families when they are faced with difficult decisions.
CPS strives to protect and promote the health and well-being of children and youth. It is consistent with this mission to protect the most vulnerable by giving them a chance and by supporting their parents.
We urge the Board of CPS to reconsider and revise this Statement with experienced parents through a collaborative, transparent process.
We would be happy to collaborate on a revision of the statement.
Sincerely
Katharina Staub, President
For the Canadian Premature Babies Foundation-
Pour la Fondation pour Bébés Prématurés Canadiens
Although this seems wonderfully supportive in many ways, it does have a negative effect on the medical community’s outlook on Trisomy children. Many times these children do live. They thrive. Yet to not support us makes it harder to receive care for our trisomy children as doctors default to influences such as this. This simply confirms decades of old and outdated information that establishes and defines care. Please think outside this box and see our children and the future choices we make for them as they grow. Look at their faces and see the love they are given. Webstagram and Instagram we have an on going project to show you this evidence of love and survival search trisomy13_trisomy18