For anyone who was at the latest PAS meeting, you probably heard about the presentation of Proprems. This is the latest RCT of probiotics, from Australia and New Zealand, using ABCDophilus, which is interestingly manufactured in New Jersey.
The authors enrolled 1100 babies less than 32 weeks gestation, they found 4.4% NEC in the controls and 2% with probiotics. This was statistically significant. The abstract downplays the results a little I think, as they had a relatively low baseline rate of NEC the NNT was 43: they state ‘Although these probiotics appear safe, between 23 and 333 [those are the 95% confidence intervals of the NNT] infants require probiotics to prevent one case of severe NEC. Probiotics may have greatest impact globally in settings with higher rates of NEC, mortality and LOS than in Australia and New Zealand.’
If you look at the data from the ANZNN in 2010 (which is publicly available), the rate of NEC among babies under 28 weeks gestation is 10.4%. So the ‘setting with higher rates of NEC’ is right under their noses.
And even if you think that 43 babies is a lot to treat to prevent one case of NEC, I am just analyzing our first 18 months data since we started routine probiotics. Under 32 weeks, on average a baby gets 23 days of treatment. Our current cost is about 15 cents a day.
That’s right, until some drug company gets wind of it and tries to get an exclusive license to supply probiotics for premies, and then charges 10000% profit (don’t laugh, it has happened before), it costs 15 cents a day to give probiotics. So on average to prevent one case of NEC or mortality in my NICU (where the NNT is 10) costs $36.
We have had a major reduction in NEC, and in the combined outcome of death or NEC, we did have a relatively high incidence before, even with high breast feeding rates, but even if you start out with a 4.4% incidence, and an NNT of 43, the cost to prevent one case is about $150. Sounds like a good deal to me.
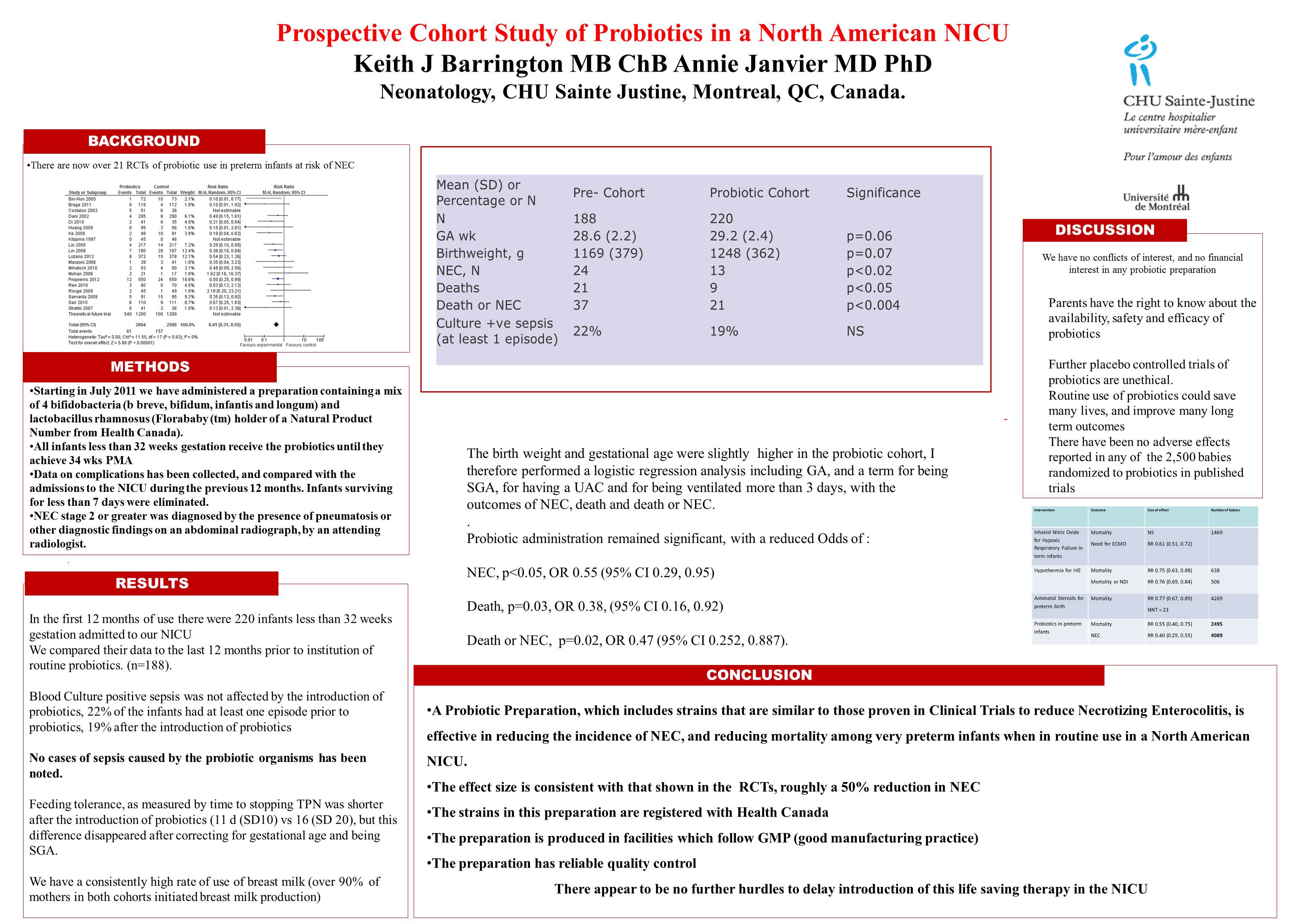
You can see below the poster of the first 12 months that we presented at the PAS meeting, the first 18 months experience are in preparation, and show even greater reductions. I will let you know when and where it is published.
Update at 1107 EST: I didn’t mention it at first but should have, in my NICU we have chosen to use Florababy, the Canadian suppliers applied for, and got, a Health Canada Natural Product Number for the product, which is reassurance of good quality control and manufacturing standards. It is a mix of 4 bifidobacteria and a lactobacillus rhamnosus, and 0.5 g per day gives you about 2 billion bugs, more or less.