Just back from a week in Panama, organised by “Wings“, mostly in Darién province at the extreme east of the country. A really amazing experience, with over 300 bird species seen, including just over 200 “lifers” for me. On my other blog, I have posted several posts, a trip report with many photos.
As a taster, this is a Collared Aracari, and below King Vultures.
Sepsis caused by organisms transmitted during, or shortly before, labour is relatively uncommon in higher income countries with GBS screening programs; the incidence is now around 0.3 cases per 1000 live births, but varies, it may be as high as 10 times that, or as low as 0.1/1000. GBS remains the commonest organism, with E Coli close behind, followed by Strep viridans, and then a host of other bugs. Early identification and treatment is the key to good outcomes.
We can think of this in 2 ways; a risk of 1 case for every 2000 births is a very low risk. On the other hand it is an identifiable 72 hours of life with the highest incidence of sepsis that one will ever have! In general terms, about half of the cases have no identifiable risk factors, and about half the cases occur in babies with a risk factor or a combination of risk factors: chorioamnionitis (or “triple-I”); maternal fever; prolonged rupture of membranes; obstetric procedures; a previous baby with GBS.
Various groups have recommended evaluating risk factors at birth in order to determine the clinical approach to be taken. Usually that means that if the risk is considered high enough, then cultures are taken and antibiotics are given, even if the infant is currently well, or perhaps strict frequent physical examination. There may also be an intermediate group, who qualify for more intensive clinical monitoring, or perhaps for lab screening tests, such as a CBC and/or acute phase reactants, CRP, procalcitonin and others.
We should think of the risk-factor-based approach just as we would any screening test for determining interventions in healthy patients. What is the sensitivity, and specificity, and, depending on the incidence in your population, what are the negative and positive predictive values, of the risk factor combination?
Risk factors are often grouped in differing ways, which makes determining sensitivity etc complex, but given that about half of septic babies lack identifiable risk factors, usually sensitivity is around about 50%.
One study from the Netherlands compared the sensitivity of the Kaiser calculator with the 2021 NICE guidelines and the most recent Dutch guidelines. (Snoek L, et al. Neonatal early-onset infections: Comparing the sensitivity of the neonatal early-onset sepsis calculator to the Dutch and the updated NICE guidelines in an observational cohort of culture-positive cases. EClinicalMedicine. 2022;44:101270), in that study, at 4 hours after birth, the Kaiser calculator had a sensitivity of 36% compared to 50% for the Dutch, and 55% for the NICE framework, among the 88 patients eventually determined to have culture positive EOS. Other publications have shown sensitivity between 37% and 76% of the Kaiser calculator, with the CDC approach being reported to have a sensitivity between 50% and 100%. See reference list below. As the babies were followed, in the Snoek study, progressively more of them developed clinical signs satisfying treatment thresholds, so that 72% were eventually “screen-positive” by Dutch and NICE guidelines, compared to 61% by the calculator. What the publication never explains is how the remaining 24 babies were picked up. Did they become sick after 48 hours? Were they screened outside of the Dutch guidelines, and if so on what basis? Did they remain asymptomatic despite positive cultures?
Overall, the calculator and other risk-based systems, in very large cohorts with current EOS incidence, will, therefore, have around about 50% sensitivity within the first 4 hours after birth. In general, more sensitive risk-factor-based approaches will, of course, screen and treat many more infants. But specificity is more variable and difficult to calculate unless you are sure about the population frequency, but if we work with an incidence of 0.5 per 1000 live births, at term or near, and that risk factor screening tags 4% of babies as being at risk, then the specificity of screening calculates to 96%, with a PPV of 0.6 and a NPV of 99.9.
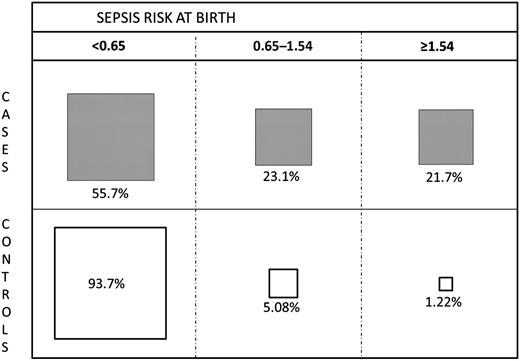
As always in epidemiology, if the risk factors are broader then the sensitivity will increase, and specificity will decrease. this is nicely illustrated by this figure from one of the studies of Escobar and Puopolo (and others), using just maternal risk factors. In this figure, higher risk at birth identified fewer cases (lower sensitivity) but had much higher specificity and fewer false positives. On the other hand it also demonstrates that the majority of EOS cases are NOT identified by their risk factors, sensitivity is <50% in the columns with intermediate and high risk of sepsis.
If we could define risk factors (or another screening test) that were more accurate, with a higher sensitivity AND specificity, then we could reduce both unnecessary intervention and false negatives. But as of now, about half of EOS cases will be among the babies that have a positive screening test result, and about half will be among the remaining infants, whether that screening test is the calculator or another one of the recent risk-factor-based approaches. The older standards were less specific, especially among babies born after chorioamnionitis, without being much more sensitive, which is why the calculator has led to a reduction in unnecessary treatment in most cohorts where it has been introduced.
For a screening test for an uncommon condition, a sensitivity of about 50% is pretty poor, and for any other condition we would probably abandon that approach! Imagine if our screens for hypothyroidism, or for PKU only had a sensitivity of 50%.
Can we make risk-factor-based screening more sensitive AND more specific?
The Kaiser EOS calculator, if strictly applied, usually ends up with about 4% of all babies receiving antibiotics. I have been trawling through recent literature (and there is a lot of it!) and, of unselected populations, the range of babies recommended to start or strongly consider antibiotics, is between 1 and 5%. That obviously also depends on the prevalence of the risk factors, one very important one being chorioamnionitis. Many guidelines that I have found steer clear of trying to define that phenomenon. They either leave it to individuals to decide whether there is a reliable history of chorio, or avoid the term and use maternal temperature instead. That widely-used Kaiser calculator doesn’t mention chorio, just highest maternal temperature. If you enter data into that calculator, the presence of a maternal fever of 39 degrees increases the risk of EOS by about 40 fold compared to a temperature of 37, depending on the other risk factors.
In contrast the NICE framework in the UK refers to a “clinical diagnosis of chorioamnionitis” but without diagnostic criteria; in full, the NICE list of antenatal risk factors is
Red flag risk factor:
Suspected or confirmed infection in another baby in the case of a multiple pregnancy.
Other risk factors:
Invasive group B streptococcal infection in a previous baby or maternal group B streptococcal colonisation, bacteriuria or infection in the current pregnancy.
Pre-term birth following spontaneous labour before 37 weeks’ gestation.
Confirmed rupture of membranes for more than 18 hours before a pre-term birth.
Confirmed prelabour rupture of membranes at term for more than 24 hours before the onset of labour.
Intrapartum fever higher than 38°C if there is suspected or confirmed bacterial infection.
Clinical diagnosis of chorioamnionitis
The NICE guidance recommends cultures and antibiotics if you have one “red flag” or any 2 other risk factors. Which includes those antenatal factors, as well as the following list of clinical indicators
Red flag clinical indicators:
Apnoea (temporary stopping of breathing)
Seizures
Need for cardiopulmonary resuscitation
Need for mechanical ventilation
Signs of shock
Other clinical indicators:
Altered behaviour or responsiveness
Altered muscle tone (for example, floppiness)
Feeding difficulties (for example, feed refusal)
Feed intolerance, including vomiting, excessive gastric aspirates and abdominal distension
Abnormal heart rate (bradycardia or tachycardia)
Signs of respiratory distress (including grunting, recession, tachypnoea)
Hypoxia (for example, central cyanosis or reduced oxygen saturation level)
Persistent pulmonary hypertension of newborns
Jaundice within 24 hours of birth
Signs of neonatal encephalopathy
Temperature abnormality (lower than 36°C or higher than 38°C) unexplained by environmental factors
Unexplained excessive bleeding, thrombocytopenia, or abnormal coagulation
Altered glucose homeostasis (hypoglycaemia or hyperglycaemia)
Metabolic acidosis (base deficit of 10 mmol/litre or greater)
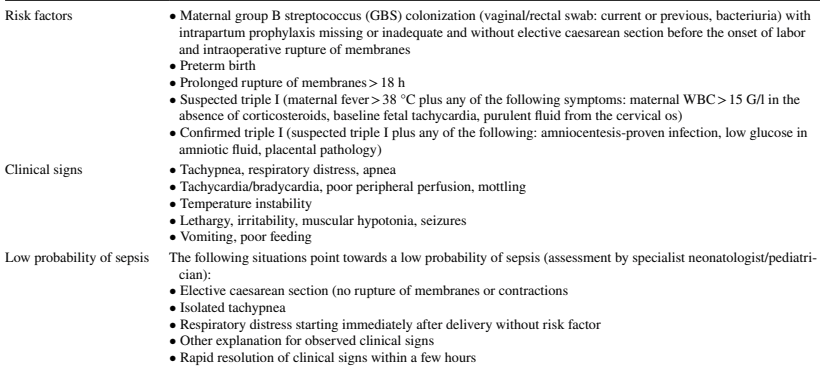
As you can see the Swiss don’t refer to chorioamnionitis at all, but use the ACOG/AAP term of triple I, which stands for “Intrauterine Infection or Inflammation…. or both” and give some criteria for that diagnosis. My only quibble with this list is that Elective Caesarean without labour or ruptured membranes has a zero, rather than low, probability of EOS, and should be listed as a contraindication to doing a sepsis workup!
Once an at-risk patient is identified, the Swiss guideline recommends Serial Physical Examination, SPE. And here it starts to get questionable, for me. For the Swiss guideline that apparently simply means vital signs q4h, which they specify as being heart rate, temperature, peripheral perfusion and skin colour. Exactly how this is meant to be done, by whom, and with what criteria, are not specified; what exactly is meant by “peripheral perfusion”, for example? If this is going to be done for thousands of babies, it is vital that it is clear and unambiguous. As I understand it, babies with a low probability of sepsis should have routine care, which, I suppose therefore, must exclude q4h vital signs.
However, the references that they give to support the SPE approach have all used very different approaches. For example, here is a figure from an Italian group (Berardi A, et al. Serial physical examinations, a simple and reliable tool for managing neonates at risk for early-onset sepsis. World J Clin Pediatr. 2016;5(4):358-64) that have published about their approach a few times. As you can see, they immediately culture everyone with “chorioamnionitis” or intrapartum fever, and, for the remaining at-risk infants, do the SPE on multiple occasions, “in turn by bedside nursing staff, midwives and physicians” using a purpose built form, shown here. The methodology and timing of the SPE is vitally important.
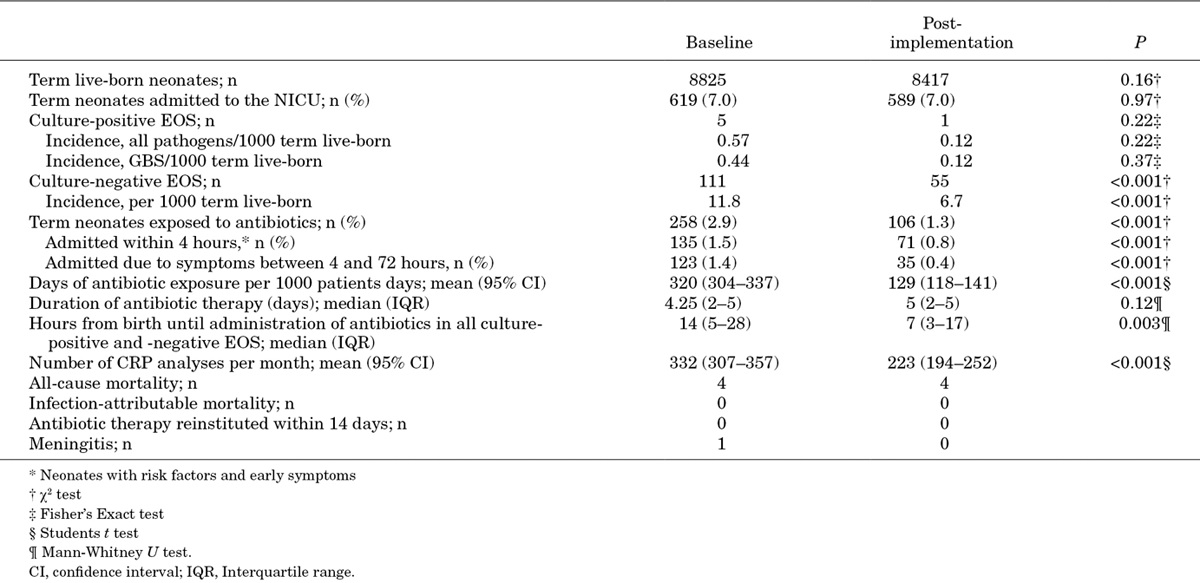
Among the 8000 babies analyzed using this approach, there was 1 true, culture-positive, sepsis (and supposedly 55 “culture-negative sepsis”), and about 1% of infants treated with antibiotics; with no deaths due to sepsis.
The group in Stanford Joshi NS, et al. Clinical Monitoring of Well-Appearing Infants Born to Mothers With Chorioamnionitis. Pediatrics. 2018;141(4):e20172056 have a different approach again, they directly observed the baby with risk factors for 30 minutes, then, in an initial phase, admitted them to the level 2 nursery on a cardiac monitor with q4h vital signs for 24 hours minimum, then transferred to maternal/infant care thereafter. In the second stage of their project, the infants went directly to maternal/infant care, and had “vital signs and clinical nursing assessments with documentation in the electronic health record at 0, 30, 60, 90, and 120 minutes and then every 4 hours for the first 24 hours after birth. After 24 hours of age, vital signs and clinical nurse assessments were performed every 8 hours until discharge. Nurse staffing ratios for all neonates in couplet care in the postpartum unit were 1:3”. The Stanford experience in that 2018 publication only included 277 infants, all of whom were exposed to “chorioamnionitis”. They showed that their approach was safe, but there were 0 cases of culture-positive sepsis, so again, I could suggest that ANY approach would have been safe!
In a much more extensive report from Stanford from 2020, there were 20,000 infants, with 6 cases of GBS sepsis, no other culture positive sepsis (and one probable CSF contaminant with 2 coagulase negative staph species). It seems that all their newborn babies are monitored in the same way, regardless of any risk factors, with the vital signs recorded at those same intervals and a 1:3 nursing ratio, for the 1st 24 hours of life. Despite the reliance on SPE, they still treat about 4% of all the term and near-term infants with antibiotics; or about 150 babies treated for every true case.
In Lausanne (Duvoisin G, et al. Reduction in the use of diagnostic tests in infants with risk factors for early-onset neonatal sepsis does not delay antibiotic treatment. Swiss Med Wkly. 2014;144:w13981) they have done things differently again, in 2 different time periods they first did the following “Vital signs were checked by midwives every 4 hours during the first 24 hours and every 8 hours during the next 24 hours in all infants with risk factors for EOS” during that period they also did CBC and CRP in all the babies with risk factors. During period 2 “in addition to the monitoring of vital signs by midwives, infants with risk factors for EOS were examined by paediatric residents every 8 hours during the first 24 hours” but they stopped doing the routine CBC and CRP.
In Lausanne, there were 11,000 babies in their report, with only 3 proven infections, which were all in the 6000 infants in the first period. None among the 5000 in the second period. Which is an example of why these decisions are so difficult to make. In the second phase of their study they could have done nothing at all, just sent all the babies home without ever examining them, and treating none of them with antibiotics, to make a silly suggestion, but as there were no culture-positive cases of sepsis in 5000 babies during that period, the results would, I propose, have been just as good! About 2% of all babies born received antibiotics.
When neonatal sepsis is so uncommon, at less than 0.5 cases per 1000 live births, we need enormous studies to prove the safety of one approach over another.
In order to really determine the risk/benefit balance of any particular approach, we need to know the real risks of each approach, with the major benefit, of course, being that we prevent death or serious illness from EOS. But, even that benefit is difficult to determine.
Imagine a well-appearing baby with enough risk factors to receive immediate antibiotics by the EOS calculator, but the baby is treated in a centre using an SPE approach without immediate antibiotics. The infant then develops a serious illness at 6 hours of age, and has a culture and antibiotics; how should that be counted? Is that a success of the SPE approach, or an unnecessary clinical deterioration? We cannot just look at sepsis related mortality, as that is extremely rare, and most of the cohorts have between 0 and 1 death.
If we use a risk-factor based approach, which identifies around 6% of babies as being at risk of EOS, and includes about half of the cases, in a population with an EOS incidence of 0.4 per 1000 the incidence among the 6% at risk will be about 0.3%; among the remaining 94% of infants EOS incidence will be 0.2 per 1000. The Kaiser calculator refines this further, dividing into a category at highest risk, including about a quarter the EOS cases. Which means that there are 1.5% of babies at highest risk, and among them the incidence of EOS approaches 1%.
The question then becomes almost philosophical, should we culture and treat those at highest risk, with the hope of preventing deterioration, but with the knowledge that 99% of treated babies will not be infected, and will have the pain, the adverse impacts on parental infant interaction, and the dramatic, long-lasting effects on the intestinal microbiome.
We also cannot eliminate the risk of EOS and a later deterioration among screen-negative babies, so must ensure adequate parental education, and some sort of surveillance of even low-risk babies.
Perhaps the best approach would be to ensure intensive clinical surveillance of the 1 to 2% of infants who are highest risk, in a way which has the least adverse impact on the infant and the family; an intermediate form of surveillance for the 4 or 5% who at intermediate risk, while ensuring that the system is fail-safe, and babies are not missed. But we must not forget the remaining 95% of infants among whom half of the EOS cases occur, and ensure some form of surveillance for that group with an incidence of maybe 0.1 per 1000. Whether that should include occasional nursing evaluation, parental education, increased sensitivity to the problem of the population at large, or some combination, I do not know. I don’t think it is feasible in most health care systems to follow the Stanford approach of “enhanced clinical monitoring” in all newborns, with frequent vital signs, nursing examinations and 1:3 nurse to baby ratio. Creating the right safety net for low risk babies will detect as many cases as screening or SPE among the high risk.
Additional References (without URL links, I ran out of steam!)
Gyllensvard J, et al. Antibiotic Use in Late Preterm and Full-Term Newborns. JAMA Netw Open. 2024;7(3):e243362. Kuzniewicz MW, et al. Update to the Neonatal Early-Onset Sepsis Calculator Utilizing a Contemporary Cohort. Pediatrics. 2024;154(4). Dimopoulou V, et al. Antibiotic exposure for culture-negative early-onset sepsis in late-preterm and term newborns: an international study. Pediatr Res. 2024. Harrison ML, et al. Beyond Early- and Late-onset Neonatal Sepsis Definitions: What are the Current Causes of Neonatal Sepsis Globally? A Systematic Review and Meta-analysis of the Evidence. Pediatr Infect Dis J. 2024. Achten NB, et al. Sepsis calculator implementation reduces empiric antibiotics for suspected early-onset sepsis. Eur J Pediatr. 2018;177(5):741-6. Coleman C, et al. A comparison of Triple I classification with neonatal early-onset sepsis calculator recommendations in neonates born to mothers with clinical chorioamnionitis. J Perinatol. 2020. Morris R, et al. Comparison of the management recommendations of the Kaiser Permanente neonatal early-onset sepsis risk calculator (SRC) with NICE guideline CG149 in infants >/=34 weeks’ gestation who developed early-onset sepsis. Arch Dis Child Fetal Neonatal Ed. 2020:fetalneonatal-2019-317165. Goel N, et al. Screening for early onset neonatal sepsis: NICE guidance-based practice versus projected application of the Kaiser Permanente sepsis risk calculator in the UK population. Arch Dis Child Fetal Neonatal Ed. 2019. Sloane AJ, et al. Use of a Modified Early-Onset Sepsis Risk Calculator for Neonates Exposed to Chorioamnionitis. J Pediatr. 2019;213:52-7. Gong CL, et al. Early onset sepsis calculator-based management of newborns exposed to maternal intrapartum fever: a cost benefit analysis. J Perinatol. 2019. Carola D, et al. Utility of Early-Onset Sepsis Risk Calculator for Neonates Born to Mothers with Chorioamnionitis. J Pediatr. 2017.
In order to put this in context, I have just been trying to search the literature for all the prior trials, knowing that there were 2 trials from Yeh’s group in Taiwan, the 2nd being a very positive trial performed in 3 centres, 2 in Tawian and 1 in Chicago. There have been several systematic reviews published, the most recent of which was published in a journal called “Respiratory Medicine and Research” and dates from June this year. In that recent SR I saw many more trials than I was aware of, and I must say, this foray was extremely disturbing. There is an enormous amount of very questionable research being published and/or referenced. Below is the Forest plot which includes both studies of early budesonide inhalation, as well as studies of budesonide instillation with surfactant. Bassler 2015 is of course, the NEUROSIS trial, which showed slightly higher mortality with budesonide inhalation, but less BPD among survivors. This Forest plot shows BPD among survivors from all the early inhaled/instilled steroid trials.
I tried to find some of the other trials. Heo2020 is actually a retrospective chart review, with no consent, and no mention of randomization. Wen2016 is from “World Latest Medicne Information” (sic) and impossible to find. Among other studies included in the SR were Cao2018, published in 2018 in the “Journal of Pediatric Pharmacy” which, as far as I can tell, stopped production in 2017, Zhou2019 was also apparently published in the same ex-journal in 2019. Kou2019 is also untraceable, with the link in the reference list of the SR leading to a completely different article.
Some of the real articles in the SR include Pan2017 (Pan J, et al. [Clinical efficacy of pulmonary surfactant combined with budesonide for preventing bronchopulmonary dysplasia in very low birth weight infants]. Zhongguo Dang Dai Er Ke Za Zhi. 2017;19(2):137-41, the abstract is in English, for the rest I used Google translate) 15 babies were randomized to budesonide with their surfactant, and 15 to surfactant alone. The incidence of BPD (defined as needing oxygen at 28 days) was 1 vs 6, which the authors claim was “significant and statistically significant”; of course, it is far from being statistically significant, by Fisher Exact, p= 0.08. Ping2019 also seems to exist, it appears to be a report of a prospective RCT, and seems to show a reduction in moderate to severe BPD, which is undefined in the abstract, which is all I can get hold of. Ke2016 is a 4 group RCT, with 46 subjects per group, one of the groups being budesonide plus surfactant, and one being surfactant alone, the others being budesonide by inhalation using 2 different methods. Yao2021 was published in “American Journal of Translation Research” and purports to be a trial using nebulized budesonide.
It is impossible to know how much of this research was actually ever performed, how much is fictional, how much was invented by AI, how much is re-quoting of numbers from other reviews without adequate checking of the original.
This is very disturbing to anyone wanting to provide high-quality medical care, based on reliable evidence, to sick babies. One way to deal with all this is that, when we write or review a Systematic Review for publication in a reliable journal, we must insist on only prospectively registered trials, with publicly available data. We will have to perform more independent IPD meta-analyses, where the review authors share, and can examine each others anonymised individual data, if we are to be able to rely on the best evidence for our patients.
The background, therefore, to PLUSS, was of a single high-quality trial of moderately large size (n=265 total), Yeh 2016, which doesn’t even appear in the Forest plot above (probably because they did not publish the incidence of BPD among survivors) but which showed a substantial decrease in oxygen needs at 36 weeks, from 50 to 29 %, which was due to a reduction in both moderate BPD (31 to 20%) and severe BPD, (19 to 9%). The RR for “BPD or death” was therefore 0.63, 95% CI 0.5 to 0.8.
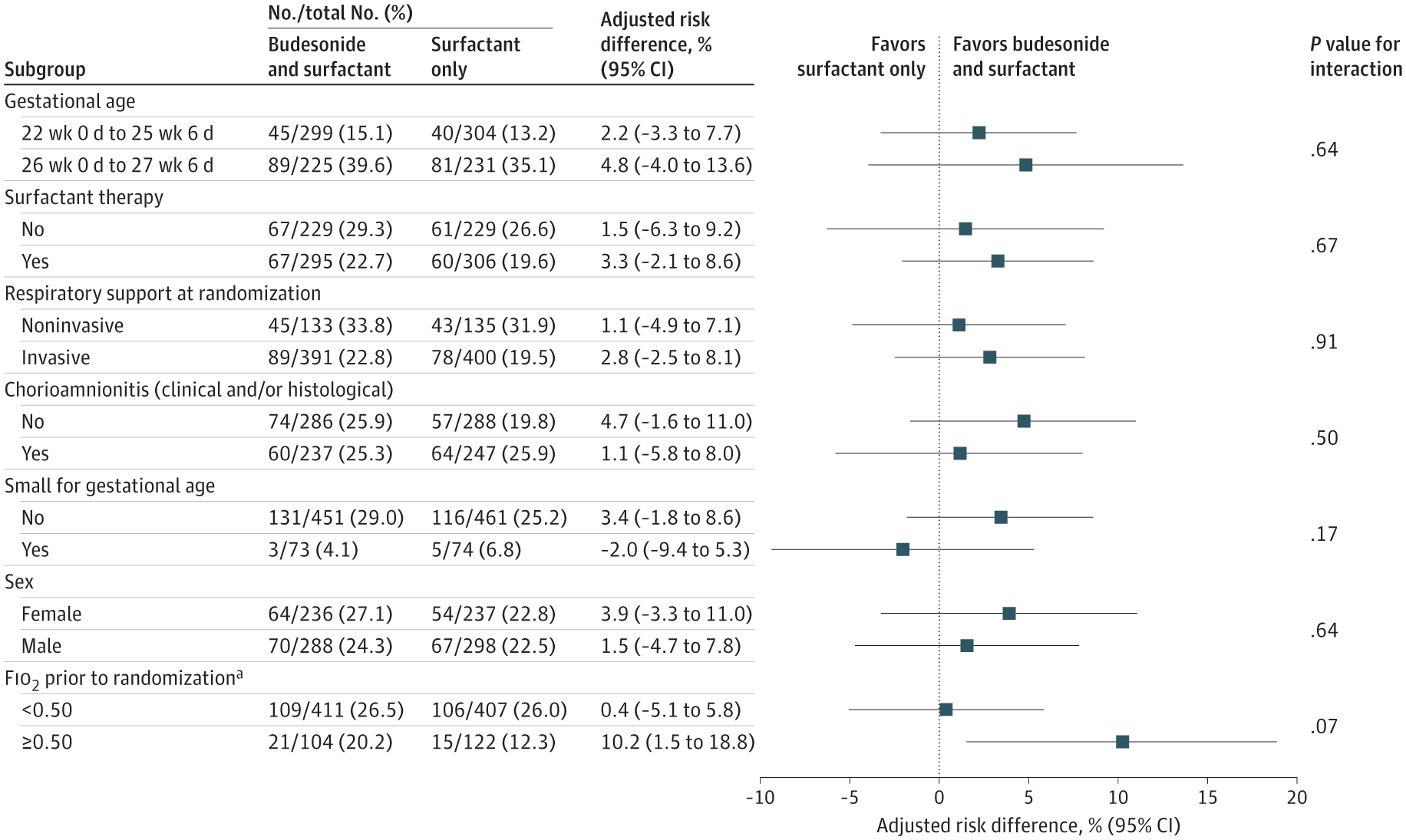
If we recalculate the primary outcome of PLUSS as a relative risk of the primary outcome, it was 0.96, with 95% CI of 0.9 to 1.03. In other words, not only was there likely no benefit, with the residual possibility of a small benefit or a minor harm, but no overlap with the CI of the previous trial either. Also of note, there was no impact of budesonide in any of the prespecified subgroups either. Only a post hoc subgroup analysis of the infants with an FiO2 >50% at treatment showed some hint of a benefit.
So why is PLUSS so different to Yeh et al? PLUSS used a different surfactant (poractant rather than beractant in the previous study) had more immature infants, (average GA 25.6 weeks compared to 26.5 weeks), who needed less oxygen on average at intervention (average of 30%, compared to a mean FiO2 in Yeh et al of 60%) and had a maximum of 2 doses of budesonide, compared to a maximum of 6 doses in Yeh’s study.
Yeh had lower mortality, and less BPD among survivors than PLUSS, in the control groups. Mortality in the controls was 16% in Yeh’s trial, and 20% in PLUSS, while BPD in survivors was 55% vs 72%.
In PLUSS, infants who had already received one dose of surfactant were eligible to be randomized at the time of the second dose, if they were still < 48 hours of age. In fact about half of the infants (in both groups) had already received a dose of surfactant without budesonide prior to being randomized. But one of the pre-planned subgroup analyses was restricted to infants getting their first dose of surfactant, and that also showed no benefit of budesonide, as you can see from the figure above, “Surfactant therapy” means previous surfactant without budesonide prior to randomization. So the ‘No’ results are for babies getting their first dose, and there is an almost identical primary outcome (Death or BPD) among these babies. Because prior surfactant treatment was permitted in PLUSS, the average age of administration of the study drug was later, at 5 hours, compared to 2 hours in Yeh et al.
The new study was much larger than Yeh, and allowed surfactant via LISA/MIST, compared to all the babies being intubated in the previous trial. The differences in outcome, with this new high-quality trial showing no benefit with budesonide, could be because of the differences I have discussed, or some other currently uncertain effect, or simply because of random variation. As I already mentioned, the confidence intervals of the primary outcome of PLUSS do include the possibility of a small benefit of budesonide instillation, but do not overlap with the CI of the trial of Yeh.
Post hoc subgroup analyses, such as the one performed here of above and below 50% O2, should always be treated with great suspicion. Introducing new, unplanned analyses after the data have accumulated is very risky, and inflates the possibility of a type 1 error, suggesting a difference which is not real. In addition, the interaction term was not significant, which means that, although the subgroups with FiO2 above and below 50% had different results, there is not a statistically significant difference between those subgroups. For all these reasons, budesonide instillation with early surfactant cannot be recommended based on this trial, even for babies with very high oxygen requirements. It may be that another trial enrolling only infants with very high oxygen requirements could possibly show a benefit, but that is a possibility that can only be answered by doing such a trial.
The BIB trial, currently underway in the USA does not, however, restrict enrolment to infants with a high FiO2, and is in many ways similar to PLUSS, with the main difference being a restriction to the first dose of surfactant, and the inclusion of infants up to 28 weeks and 6 days gestation. BIB has completed enrolment, and, you never know, perhaps we will see some results at PAS next spring. Once we have those results, we should be able to make an evidence-based decision about routine budesonide instillation with surfactant, and we will be able to ignore all the very small, potentially unreliable or perhaps fictitious trials in the current Systematic Reviews. Perhaps, if someone has the time and the funding, we could do an IPD meta-analysis, and only those investigators who are able to supply the individual patient data, from pre-registered trials, could collaborate to give the best possible information for future babies, and for future trials.
As usual for a TED talk this is 18 minutes long, and, in that brief time, Annie recounts her trajectory: learning from families of kids with trisomy 13 and trisomy 18; our own experience with counselling for threatened extreme preterm birth, from both sides of the conversation; and the Parents Voices Project. The only thing I don’t like about this video is the still that was chosen by their algorithm to appear with the title, which has a weird expression on Annie’s face.
The description below the video of Annie’s TEDx talk, which she presented in Fort Lauderdale in September this year, at the Delphi conference of neonatal innovation, notes:
In this heartfelt TEDx talk, Dr. Annie Janvier, Professor of Pediatrics and Clinical Ethics at the University of Montreal, shares profound insights from her work as a neonatologist and ethicist. Drawing on her personal experiences as a mother to children with healthcare needs, including one born at just 24 weeks, Dr. Janvier explores the lessons that premature and critically ill babies can teach us about resilience, life, and the complexities of healthcare. Her unique perspective sheds light on the challenges families face and the ethical questions that arise in critical care, encouraging us to view life and health through a compassionate lens. Dr Annie Janvier is a Professor of pediatrics and clinical ethics at University of Montreal. She is neonatologist and clinical ethicist at the Sainte-Justine University health center. She holds a PhD in Bioethics and co-directs the Masters and PhD programs in clinical ethics at University of Montreal. She works first hand with patients and families confronted with difficult decisions such as end-of-life issues, and decision-making in the face of uncertainty. She is also the parent of three children who had or have healthcare needs, one of which was born at 24 weeks
The most recent publications from the Parents’ Voices Project include
There are only a few randomized trials in neonatal surgery, but those that exist have had a major impact. This new publication may do the same, even though the sample size is relatively modest, and there are some issues with the article. You can see some of the difficulties in doing such trials from the fact that it took 12 hospitals 9 years to recruit 80 patients, 58 of which came from only 3 of those hospitals, Sick Kids, GOSH, and University Children’s Hospital in Belgrade, the others having between 1 and 5 patients each. (Eaton S, et al. STAT trial: stoma or intestinal anastomosis for necrotizing enterocolitis: a multicentre randomized controlled trial. Pediatr Surg Int. 2024;40(1):279).
The investigators enrolled infants with NEC prior to surgery, and randomized them during the procedure if they felt that either enterostomy or primary anastomosis were both reasonable surgical options. After elimination of one subject who had been randomized twice, they had 79 patients enrolled, with 42 having a stoma and 37 a primary anastomosis. This appears to be a very reasonable trial approach, where the individual surgeon has equipoise at the moment of surgery.
The first problem with the trial is that there were 6 patients lost “to all follow up”. I don’t understand how it is possible that the authors don’t even know if they survived or not. If there were big problems with record-keeping in some centres maybe the primary outcome variable, ‘days on parenteral nutrition’ might be difficult to find years later. But this was a prospectively registered trial, so it is not clear to me how simple data, easily available during the initial hospitalisation, can be missing on 7% of the subjects.
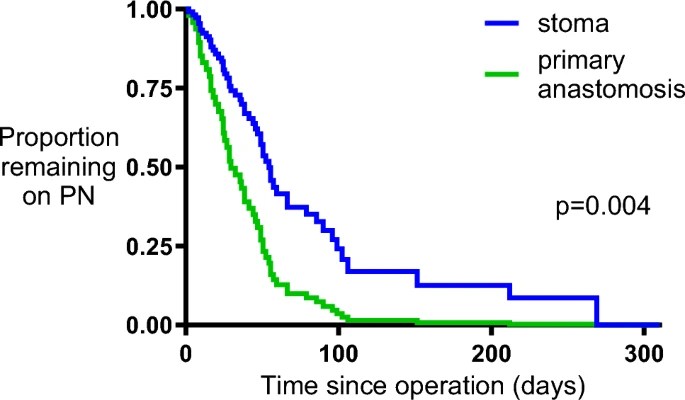
There are other significant problems with the manuscript. The primary outcome was, as mentioned, days on TPN, but how the investigators dealt with mortality in this outcome is not at all clear, the results present the primary outcome among survivors initially, which was a median of 51 days (range 3 days to 4 babies still on TPN at the end of follow up 310 days) among the stoma babies, and 30 days (range 4-105). They then present an analysis by an adjusted Cox regression, censored for mortality. As noted, they state in the text that 4 stoma babies were still on TPN at the end of follow up, but the figure shows everyone as being off TPN before 300 days.
The survival curves are also strange. There were only 4 deaths in the primary anastomosis group, but the curve seems to show about 13 steps down in the survival curve, and both curves continue to show deaths up to 200 days, this isn’t because some patients haven’t yet reached the final follow-up as that was completed in January 2020, and there were no further losses to follow-up in the anastomosis group at 3 months or at 1 year. The curves seem to suggest that the final proportion of the stoma patients surviving was 0.8, but there were 4 deaths of 35 with known outcome, which leaves a proportion of 0.88 surviving.
While keeping all of these concerns in mind, the results do seem to show major advantages of primary anastomosis, with the duration of TPN among survivors being shorter, and there being more survivors, 8 deaths in the stoma group vs 4 after anastomosis.
It would be interesting to see whether the experience with the stoma patients in the trial is similar to other patients having a stoma outside of the trial. It seems to me that the fact that 10% of the stoma patients were still on TPN at one year of age, when they were already a selected group, who were relatively stable and with relatively restricted disease, is a surprisingly poor outcome. There were substantially more complications in the survivors in the stoma group, with more wound infections, and, of course, more stoma complications, than among the survivors in the anastomosis group.
The study report may have a lot of big problems, but it does at least suggest that immediate primary anastomosis is a very viable approach in infants who are stable enough to have it considered, and in whom the distribution of disease makes it feasible. There may well be fewer post-op complications with anastomosis, and the number of later strictures were similar between groups.
As some of you may have noticed, I left Twitter (X), apart from sending a link to each new post on this blog. I never any longer visit the website and I have deleted the App on my phone.
A great alternative is the nicuverse, nicuverse.org a Mastodon community with many similar functionalities that we could use to chat with each other, discuss research and clinical approaches. You will see also that there are links there to another on-line community 99NICU. They recently organised a conference in Portugal, much of which is available on-line, and they have a YouTube channel which has numerous videos of presentations from that conference. Several of which I have watched, and they are all of high quality.
For example, in keeping with some of my recent posts, there is a very good presentation about the use of antibiotics and the evidence-base for our current practices.
Another, about what on earth should we do about the PDA? Has 3 stellar presenters rather than just one!
One of the reasons for mentioning this now, is the upcoming series of Webinars about, and by, adults born preterm. You can register for them, or, I am sure, watch them later on-line. One of them is embedded below.
Rethinking the definition of clinical research, and how we approach the essential protections of research subject is clearly needed.
In my NICU, if I have a 3 week old preterm baby who develops signs of septic shock with poor perfusion and a low blood pressure, in general my approach would be to give a bolus of normal saline (10 mL/kg) over a fairly short time, then to start a norepinephrine infusion, and usually start low dose steroids very early. I would start norepinephrine at about 0.1 mcg/kg/min, often the response is slow, and I may increase to as much as 0.4 mcg/kg/min before, often, being able to back off fairly quickly as the steroids and antibiotics have their effect.
Were those publications “research”? We described our practice and the outcomes, in the hope that others will evaluate their own practice and compare with ours, and we had local ethics approval to go through the databases and publish our results. In another NICU, they might routinely give multiple fluid boluses, followed by dopamine, and only use steroids as a last resort. Also without a good evidence base. As each baby is so different to the last, observational studies have limited value. It is, indeed, very hard to imagine how comparing these approaches and determining best practice is possible, even with all the fancy statistical adjustment in the world, including the latest version of propensity score matching, unless large randomized trials are performed.
I can treat babies in this non-evidence-based way, and then compare with other approaches, or change my practice and then re-evaluate, with almost no oversight, and certainly no prior IRB approval. What if I wanted to do something much more scientifically valid, such as trying to standardize therapy as much as possible, then prospectively comparing the outcomes from my centre to other centres that have also tried to standardize their treatment approaches? Then, even if every baby gets exactly the same therapy as they would have done anyway, does this suddenly become a research study? The CNN, Canadian neonatal network, are actually doing such a study, in which centres who usually use norepinephrine for septic shock, and those who use dopamine try to standardize their initial treatment, and we will compare outcomes.
A much more valid study, and one which would cost much more, and be substantially more difficult to organise, gain approval, and perform, would individually randomise eligible babies to one approach or the other. An intermediate type of study, where NICU’s are randomized, has some advantages in terms of, for example, ensuring the team is familiar with the approach over time, and not requiring masked vials of study drug; but has major impacts on sample size. Either a cluster-randomized or individually randomized trial will require prior IRB approval.
One big question for an IRB is how to determine the risk of such a study. In the past, because there is a substantial risk of death, and of major complications, this should be labelled as a high risk study. The risks of a participant in the study are much greater than the risks of daily life, even of daily life of a preterm baby in the NICU. Surely, though, the risks of the research project should be a comparison of the risks of adverse outcome if you are in the trial compared to being not in the trial. What matters is whether there is additional risk over not being a study participant. Clearly, in the scenario I have described, the risks are identical to not being in the study. It should be considered as “no additional risk”.
The new Declaration of Helsinki does not go into any detail about which risks to include in evaluating a research project. It states that a project must be “preceded by careful assessment of predictable risks and burdens to the individuals and groups involved in the research in comparison with foreseeable benefits to them and to other individuals or groups affected by the condition under investigation.”
The discussion by Kass et al puts it this way: “Our specific recommendation here, with relevance for comparative effectiveness and other types of research on approved or widely used clinical approaches, is for oversight bodies to make their risk-level determinations, including whether a study qualifies as minimal risk, on the marginal or additional risks and burdens of research participation, relative to those of ordinary usual care.”
An accompanying editorial in JAMA points out how these proposals differ from current rules. According to OHRP current rules, “in general the reasonably foreseeable risks of research in a study include the already identified risks of the standards of care being evaluated as a purpose of the research when the risks being evaluated are different from the risks some of the subjects would be exposed to outside of the study”. In other words all possible risks of being a preterm baby in the NICU with septic shock undergoing intensive care are considered study risks. Which means that all possible adverse outcomes of the extremely high-risk situation are included, death, IVH, renal failure, and so on. That interpretation of the OHRP rules makes intensive care research just about impossible, as it requires the IRB to ascribe all the risks of being critically ill to the trial, even if there are no additional risks compared to not being in the study. I think that many IRBs already interpret the risks of a trial as being those additional risks, and I can only hope that this interpretation will become widespread.
Another question is about consent. Normally, I do not share with parents all the many the uncertainties regarding the best approach to septic shock, I do not ask them to make an informed choice between norepinephrine and dopamine, I don’t counsel them about the uncertain role and timing of steroids, and get them to sign a consent form. If I am planning to prospectively collect the data, with the explicit intention of comparing outcomes with dopamine centres, does that now require specific informed consent? Even though I am doing exactly what I would have done in any case? Indeed, so are my comparison centres, who use a different approach.
I think that this does not require specific informed consent, I am not even sure that we should obtain consent to contribute the baby’s data to a truly anonymous database for future comparative analysis.
What if I decide, for a while, to switch my approach to using dopamine, and collect the data, because I understand the uncertainty involved, and I think that dopamine is an equally valid choice? And my comparison centres will also switch to using norepinephrine. According to this new discussion article:
(Informed consent is required if)… the research removes from patients the ability to make a decision that may be meaningful to them—a decision that, in ordinary clinical care, they may have been invited to make.
They go on to note :some commentators support the view that consent can, ethically, be waived when risks are low and when consent is typically not sought for either approach being studied, others oppose complete waivers of consent requirements in some or all circumstances. Importantly, most of these critics of complete waivers support streamlined approaches to consent for these lower-risk, randomized studies.
In this situation, parents would not ordinarily be asked whether they prefer norepinephrine or dopamine, so the first criterion does not apply. However, my initial intervention choices are being determined by a written protocol, I think this should require that I tell the parents that their infant is getting a therapy determined by a protocol, a therapy which is, nevertheless, within the usual range of good clinical practice.
I don’t think it is appropriate to perform prospective comparative research, even with zero additional risk, without informing the parents. It seems to me to be hiding important information from the parents, and that is likely to create distrust.
I propose for such a study that consent should be altered to focus on informing parents of the important details of the study, and giving them an opportunity to opt-out of data collection. A 2017 article refers to this as “targeted consent”, whereby patients who are individually randomized to one of two reasonable, clinically appropriate treatments have a verbal information sharing session, and a brief targeted consent form outlining the patient’s rights. I don’t think that a cluster-randomized trial should be considered to be morally different, if all patients admitted in January have one approach, then in February we switch to another approach, from the patient’s point of view this is identical. Or if NICU A is randomized to dopamine, and NICU B is randomized to norepinephrine, and then switched over after 6 months. In each situation we are performing pre-planned research, and parents should know about it, and have the chance to opt-out of information collection, and even from non-essential aspects of the care protocol if there are any.
Of course, as always, if I have a valid reason to believe that this particular patient would benefit from norepinephrine, then I am morally obligated to do so, and treat them as a protocol violation, or a non-enrolled subject.
If I was to introduce levosimendan, however, a drug with almost zero use in the NICU, and no experience in the preterm infant with septic shock, then there would be a possibility of a major impact on important clinical outcomes, and the study should have completely different, and more extensive requirements and consent process.
After the dopamine and norepinephrine study finishes, it may be found that mortality is higher in one group or the other, or the incidence of a major complication differs between groups. I don’t think we can then, in retrospect, suggest that the risk of the trial changes.
This is what happened with the SUPPORT trial, where the 2 oxygen saturation target ranges, both considered to be acceptable within usual clinical practice were prospectively randomly compared. Outside of the trial and infant could have been treated with either of the 2 approaches, so, according to the standards that I am promoting here, this would be considered a trial with no additional risk. In fact, as we all know, we found a higher mortality with the lower target range, which created a storm, and was largely responsible for the OHRP guidance which I quoted above.
But, if it turns out that norepinephrine babies have a lower mortality in our study, even after correcting for every baseline imbalance possible, that does not change the a priori risk assessment of the study. To think otherwise requires some sort of magical thinking, that things which are unknowable because such a trial has never been done, should have been known before the facts existed.
Building cluster randomized comparative effectiveness trials on top of existing databases, such as the CNN, will allow us to improve therapy for future babies, with no additional risk to our current patients, and the chance of major benefits for the next cohort.
Since at least 2013 the World Medical Association Declaration of Helsinki has mandated registration of clinical trials prior to enrolment of the first subject. Since 2005 the International Committee of Medical Journal Editors has required trial registration as a condition of publication, before the onset of patient enrolment.
This principle is reiterated in the new version of the declaration of Helsinki, just published and discussed in many places, including JAMA.
Nonetheless, retrospectively registered trials are still being accepted by journals, most of whom should know better, as well as publications with no mention of registration at all. It has been a recurrent problem in some neonatal studies, and some large recent neonatal trials were retrospectively registered after being completed, and after all the data were collected. The fact that prominent journals will still sometimes accept such research gives the publications a credibility which is not deserved.
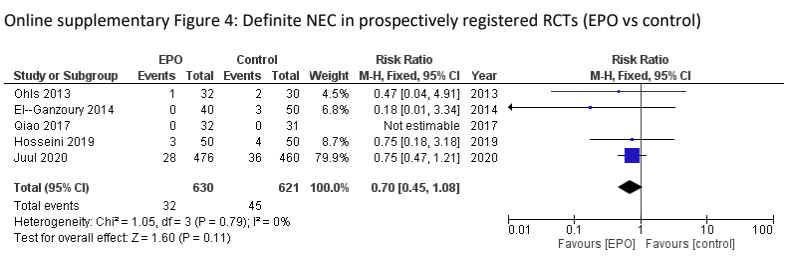
This has a significant impact on how we analyse the literature and make therapeutic decisions. To take one example, the use of Erythropoietin in preterm infants. Let’s analyse the literature to determine if Epo prophylaxis decreases NEC, a major health issue in these babies. A recent high-quality systematic review was published by Ananthan et al, Ananthan A, et al. Early erythropoietin for preventing necrotizing enterocolitis in preterm neonates – an updated meta-analysis. Eur J Pediatr. 2022;181(5):1821-33. This SR found 22 studies with over 5000 patients enrolled, and a clinically significant reduction in “definite” NEC, RR 0.77 0.61-0.98. However, of the 4 largest trials in that review 2 were registered after completion of enrolment (Song 2016, n=743, Wang 2020, n=1285), one was registered in 2006, shortly after the first patients were enrolled in 2005 but prior to completion (Natalucci 2016, n=365) and one was registered prospectively (Juul 2020, n=936). If we re-analyze the data excluding the retrospectively registered data, and the older non-registered trials, the effect of Epo on NEC no longer reaches classical statistical significance
It does still look like there might be an effect, doesn’t it? Adding Natalucci back in (the absolute requirement for prior registration dates to around the time the study was started, so it is much less of an issue) makes little difference, as they had only 3 cases with Epo and 4 in the controls. Which points out how desperately important this is. Are we failing to provide an effective therapy for our babies? Are we at risk of dosing thousands of babies with a prophylactic intervention which is ineffective?
One characteristic of many of these retrospectively registered trials is they are not published in the typical neonatal/pediatric literature, Wang 2020, for example was published in the Journal of Translation Research. Song 2016 was published in Annals of Neurology, which claims to follow the ICMJE guidelines and the declaration of Helsinki, but clearly failed to do so for this article.
I’m not sure what to do about this on-going problem. If it was bench research we could just refuse to publish, but when babies have been subjected to research procedures and parents to the stress of having a baby in an NICU and in a trial, it seems unfair to those research subjects to categorically refuse to publish. But, unless there is some sort of sanction, this will continue, and indeed it does continue. Perhaps there should be a separate journal: “The Journal of Unregistered Research”, or a separate section in some journals: “Unreliable Information”. We can’t ascribe ignorance to the authors, Song et al, who retrospectively registered the first trial in 2016 are the same authors as Wang et al, who retrospectively registered that later trial in 2020! There are numerous other problems with these 2 projects, they were unmasked trials but the controls still received placebo injections, why on earth would you do that?
The importance of trial registration is discussed in many different places, including by the WHO, one thing that the WHO don’t discuss, but which is vitally important, is that prior trial registration makes it clear if primary outcomes have been changed, or if outcome definitions have been “adjusted”. Even better is full publication of the trial protocol, in addition to registration, which makes those things even clearer, and less liable to fudging the results.
The problem is not, it seems, going away. Which may, in part, be because of the proliferation of biomedical journals, some of which have very loose standards it seems. The journal “Biotechnology and Genetic Engineering Reviews” of the Taylor and Francis group, has just published what appears to be a clinical trial of caffeine in preterm infants. (I won’t add to the hit count of the journal by providing a direct link, but the article is listed on PubMed if you want to read the abstract: Jiang Q, Wu X. Effect of early preventive use of caffeine citrate on prevention together with treatment of BPD within premature infants and its influence on inflammatory factors. Biotechnol Genet Eng Rev. 2024;40(3):2730-44). A clinical trial in newborn infants is way outside of the apparent aims of the journal, which you can read on the website. I wonder if the journal was picked at random, or because it was known to have lax editorial standards, and/or if the article was refused in other places first. None of the named editorial board members has a medical background, (it also takes on average 209 days from submission to first decision, so stay away!) As it is not a medical journal, there is no mention of the ICMJE in the descriptions I found. It is an open-access, pay to publish journal, maybe it was cheaper than other alternatives.
Not only is this the wrong place to have published this article, it is written in very bizarre English, and has very questionable features to its design. Infants were “chosen and segregated within control and observation groups through random number table protocol” which led to two groups with “no significant difference in perioperative data” and then received caffeine by “intravenous pumping” or saline.
According to the methods, apparently “Doctors and nurses should show enough patience and love in the face of children, speak gently, smile and communicate with children, try to calm the children’s mood, so that the treatment can proceed smoothly”. Who can disagree with that?!
There is no mention of ethical review board approval.
The study was apparently performed without any funding, even though there was blood work, lab analyses, respiratory mechanics equipment and procedures, and repeated neurodevelopment testing. Several inflammatory markers (MMP-9, TNF-alpha, TLR-4) were measured prior to and after therapy. TLR-4 is of course a transmembrane receptor, so I have no idea if measuring circulating concentrations is of any interest, and the results they report are 10 fold higher than any others I have found in the literature. Also it required multiple blood samples, with the pain involved.
The authors give data for respiratory mechanics, which are almost certainly fictional, as they describe no methodology for measuring mechanics (resistance, compliance and work of breathing), which is extremely difficult in any case in spontaneously breathing newborn infants. The company that they claim made the equipment they used for lung mechanics lists no such equipment on their website.
Even more bizarrely, they report the neurodevelopment of the babies which was “evaluated by Child Development Center of China (CDCC), including Psychomotor development index (PDI) and Mental development index (MDI), with scorings ranging across 0–100 points for each part”. They give results at baseline before treatment as well as after treatment (age not specified). No actual results are given, just a p-value claiming that the caffeine group had better MDI and PDI after therapy, but not the controls. The figure of these results, figure 3, is actually the same as the figure for growth, figure 4, and shows length, head circumference and weight gain.
The desperately bad research described here makes me hope it is actually a work of fantasy, as the idea of subjecting real babies to such an awful protocol horrifies me.
A huge concern is how an apparently legitimate publisher and the editorial board of this journal can allow this garbage to pollute the medical literature. I have written to the company, Taylor and Francis, (there is apparently not currently a chief editor of the journal) and left a comment on PubPeer. If any of my gentle readers have a link with Taylor and Francis, maybe you could try to trigger a response, and hopefully a retraction, before these data get incorporated into Systematic Reviews.
I started writing this post because I wanted to discuss the new version of the Declaration of Helsinki. You will have to wait for the next issue!
I think that 4 days of treatment, for a well baby with risk factors who has negative cultures, is already far too long, the optimal duration for such a baby would be 0 days! But, given that there was enough concern to perform a blood culture, then antibiotics can be stopped after 36 hours, with only a tiny possibility that a true-positive blood culture will become positive after 48 hours, and then very rarely for organisms treated with our usual empiric antibiotics.
But what about those babies who are thought to have “culture-negative sepsis”? In this new study, babies treated with antibiotics for 5 days or more, one extant definition among many, were 20 times more frequent than true EOS. There were 8000 babies with negative cultures who received treatment for >4 days, compared to 375 with a proven EOS.
What are we treating, when we continue antibiotics despite negative cultures? I well remember some twins (more than 1 pair) where one twin was sick with sepsis and positive cultures, and the other was similarly sick, but with negative cultures. To me, those cases have been the best proof that culture-negative sepsis does indeed exist. But what is it? Many such infants do not have an active bacterial infection. Many have circulatory and respiratory illness caused by the inflammatory cascade following a bacterial infection. Some cytokines have been shown to cross the placenta, such as IL6, for example, so the infant could become passively ill as a result. In other cases the infection may already have been effectively treated, such as when a mother had chorioamnionitis, and has received antibiotics. In such a case the infant is affected by the cytokines and other inflammatory mediators released by the mother or by the infant themselves. In the example I gave at the beginning of this paragraph it may be that a truly infected co-twin sets up enough of an inflammatory response that their sibling is symptomatic.
In such an infant, blood cultures will be negative, but also they will not benefit from antibiotics. The sensitivity of current culture techniques are such that, down to about 1 CFU/m, over 98% of cultures are positive, and any concentration of bugs higher than this will rapidly make the culture machine alarm ring.
For a more complete discussion of the issues in “culture-negative sepsis” you could do no better than to read Joseph Cantey’s article from the Journal of Pediatrics in 2022. I can’t tell if it is open access, but if you have difficulty getting it, I am sure we could find a way to get a copy to you.
I mentioned, in the part 1 post, another recent publication, with probably some overlap in the data, from a national Swedish database (Gyllensvard J, et al. Antibiotic Use in Late Preterm and Full-Term Newborns. JAMA Netw Open. 2024;7(3):e243362). In that publication the incidence of EOS had fallen over time up to 2020, and treatment of culture negative infants had decreased also, but the gap had actually widened. Also, in that study, the median duration of antibiotic treatment among all infants with negative cultures was 5 days, IQR 3-8 d, 97% of infants who received antibiotics had negative cultures. It is clear that not all infants who have a culture taken and are started on antibiotics have sepsis, culture-positive or -negative. Although there do not appear to be national Swedish guidelines for when to screen for and treat neonatal sepsis, there are guidelines about when to stop them (again translated by Microsoft Word)
Full-term child with suspected early onset sepsis (illness before 72h): discontinue antibiotics after 48-72h and do not diagnose as neonatal infection: • Never required ventilator care or had septic shock • Mother not diagnosed with obstetric infection • Blood culture negative, growth of contamination or not yet responded to • Well-being at 48-72h age • CRP peaks below 60 mg/L, and CRP decreases during antibiotic withdrawal • CRP peak between 60-100 mg/L, and CRP in decreasing consider discontinuing antibiotics
The way I understand it, you need all of those in order to stop the antibiotics; thus, ongoing treatment of increased CRP concentration without other signs of infection is recommended by this guide, a practice which has no evidence-base, and leads to major over-treatment of uninfected babies. Previous publications have shown that you can stop measuring CRP, and routine CBCs, without any adverse impact, only a reduction in unnecessary antibiotics. Although the Swedes are doing much better than most of us in reducing the number of antibiotic courses administered, they are still treating 50 babies with antibiotics for every truly infected infant, and as noted, they treat for a median of 5 days. If they just stopped doing CRPs, but still used the other criteria in that national standard, they could do even better, and there is no evidence that there would be any risk involved. It is well known that CRP concentrations increase several hours after the initiation of inflammation, so they are usually ignored if they are low during the initial sepsis evaluation. They also increase easily and are very non-specific, so they should also be ignored in later analysis of whether an infant has “culture-negative sepsis” or not.
There has been a lot of woolly thinking about this. Infants are defined as having “culture-negative sepsis” if they are treated with 5 days or more of antibiotics. Studies have then shown that infants with “culture-negative sepsis” have higher CRP concentrations, and this is published as evidence that CRP concentrations are useful in the diagnosis of the phenomenon. But, it is often the high CRP which leads to the prolonged antibiotic use. Circular reasoning anyone?
One early study of the neonatal use of CRP, for example, showed that 9% of the babies who were considered “definitely not infected” had raised CRP. Infants delivered vaginally have higher CRP than those delivered by Cesarean, especially CS without labour. Infants with a final diagnosis of TTN have higher CRP, as do those with Meconium Aspiration, who are often treated with prolonged antibiotics in the absence of other risk factors for sepsis. In part, this is probably because CRP increases to a mean of over 40 at 48 h in such babies, despite negative cultures and no evidence of any benefit from antibiotic use.
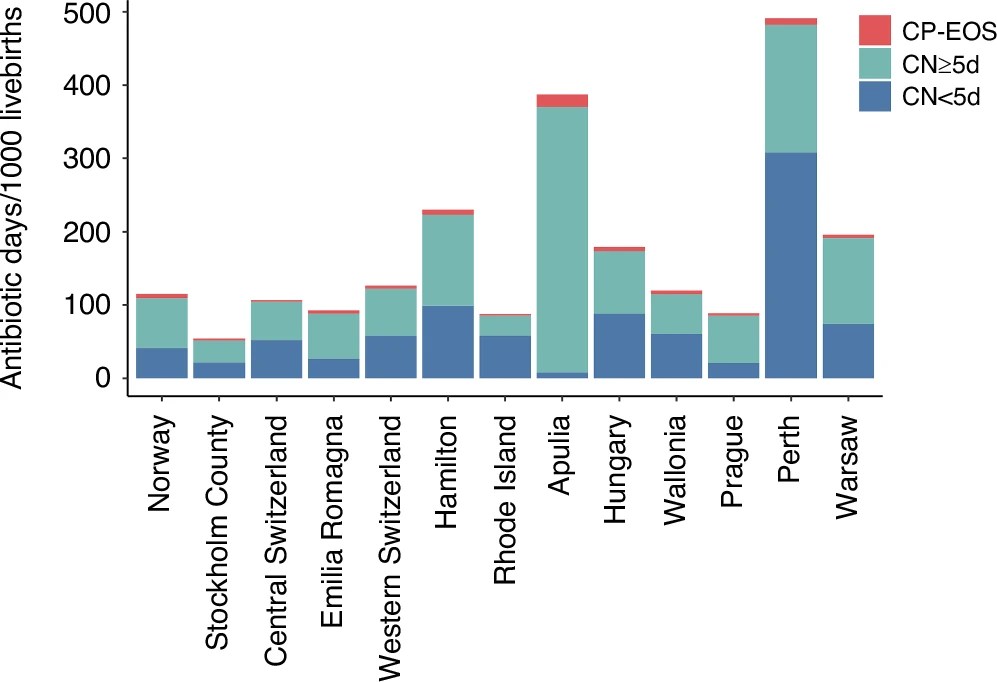
As this figure from the new article shows, the babies who clearly do need antibiotics, in red, are vastly outnumbered by the others, both the group with <5 days antibiotics, and those with 5 or more days. And there is enormous variation between networks.
Routine stopping orders for antibiotics after 36 hours, and requiring a conscious decision to continue if cultures are negative, could immediately have a big impact on exposure. A re-evaluation of each case, and a thoughtful answer to the questions “does this baby really have “culture-negative” sepsis?” and, “is this baby likely to benefit from continued antibiotic therapy?”, which are linked but not identical questions, could further reduce the unnecessary overuse of antibiotics. It would help to preserve their usefulness for the future, as well as reducing adverse impacts on that individual.
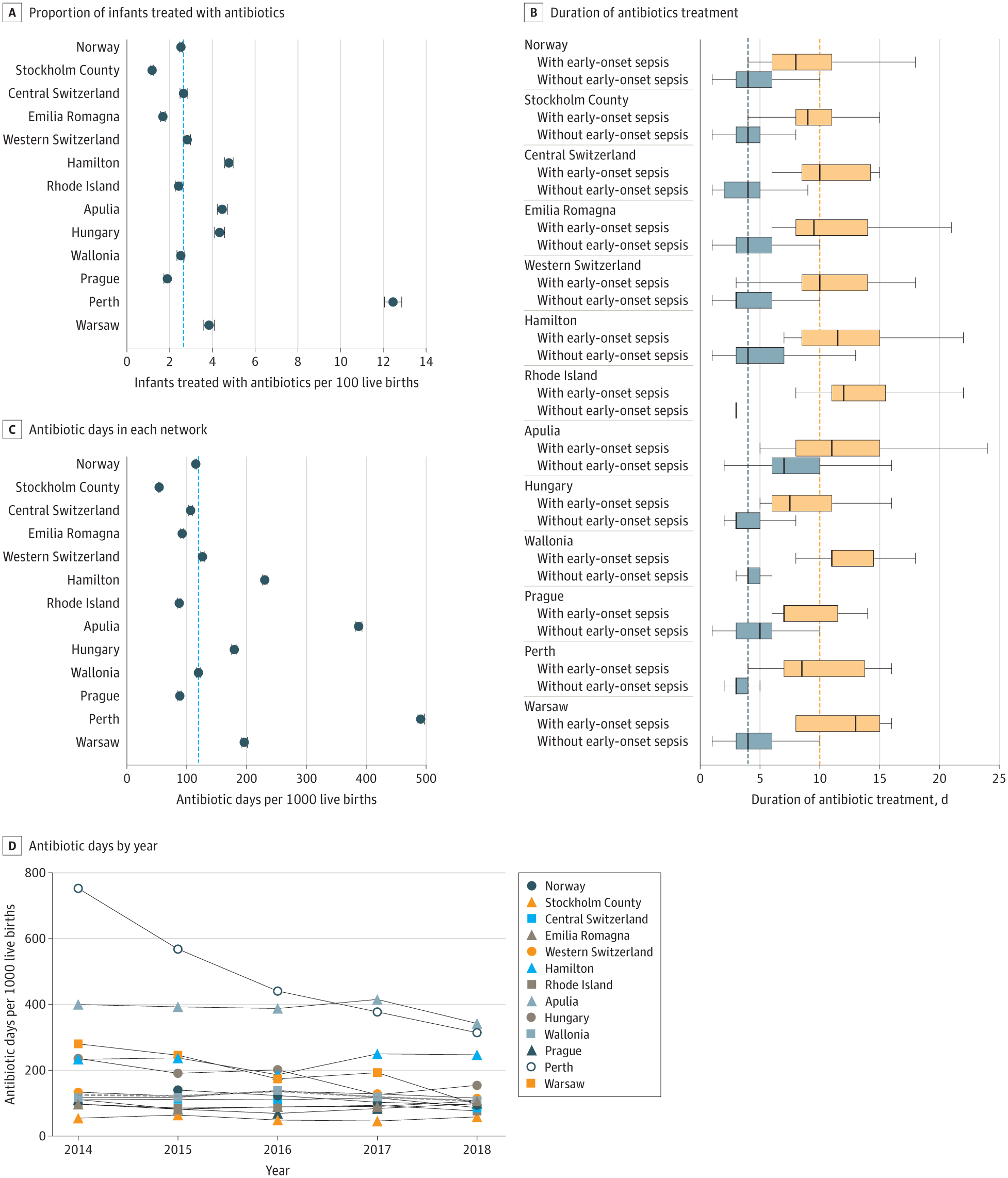
An important multi-centre observational study examines how many newborn infants, term or late-preterm are receiving antibiotics, for how long, and the responses to negative cultures. Centres from Europe, Australia and North America are represented. Data collection differs between the participants which are all regional networks (or in the case of Norway, national), but all provided data on babies who received antibiotics for any reason within the first week of life.
The overall incidence of culture positive sepsis was less than 0.05%, if the coagulase negative staph are eliminated (they were not automatically considered to be contaminants in this study, but I think it is very rare that EOS in term and late preterm infants is really caused by CoNS) the incidence was 0.041%.
One thing I really appreciated in this publication is the openness of the investigators to identify themselves. As you can see below, the centre with the highest exposure of babies to antibiotics was Perth. As you can also see, from panel B, they, and Rhode Island, are the sites with the shortest duration of treatment of culture negative babies. As you can also see, panel D, Perth dramatically reduced antibiotic exposure between 2014 to 2018.
Figure 3 in that publication shows a vague correlation between actual sepsis incidence and antibiotic use. In the supplement there is a version without CoNS
I find it hard to believe that individual decision making about sepsis evaluations and antibiotic treatment are affected by a difference in true EOS rate between just over 1 per 1000 compared to 0.3 per 1000. But, perhaps, the local choice of which guidelines to follow is affected by sepsis rates?
In terms of the consequences of sepsis, EOS mortality was very low, at 3.2% of the true EOS cases, or 12 deaths among 750,000 babies. As you can see from the figures, Stockholm county has an average incidence of EOS, but consistently has the lowest rate of antibiotic treatment. They do this, it appears, by not using the Kaiser Permanente sepsis calculator. That calculator has reduced antibiotic use in centres where it has been introduced, but the lowest antibiotic use reported after introduction of the sepsis calculator is 3%. In Stockholm the rate is less than half of that. How do they do it, without an increase in sepsis mortality? As far as I can tell, there are no published guidelines in Sweden regarding when to screen and/or treat the term and late preterm infant for sepsis. I downloaded and translated the national recommendations, but they only discuss the antibiotics available, the importance of blood cultures, a statement that culture negative sepsis is a possibility, and a vague discussion of epidemiology. This is the automated translation (Microsoft Word) of the section about screening and diagnosis:
Underdiagnosis of severe neonatal infection can quickly lead to a worsening situation of septic shock and even death, while overdiagnosis can lead to unnecessary antibiotic use. Fatigue, poor skin color, episodes of apnea, and bradycardia are common symptoms of sepsis.
Using hands, eyes, ears and stethoscopes to examine the patient and interpret these symptoms is and remains the basis of all diagnostics. In addition to this, the doctor has a number of diagnostic methods available, each with its different strengths and weaknesses (Table III). There is currently no method that has optimal speed, sensitivity and specificity. CRP is the most commonly used diagnostic test.
Another recent publication of national data from Sweden, which includes over 1 million babies and extends until 2020, shows a continuing low frequency of antibiotic exposure, with a decreasing incidence of EOS. Again, in that publication there is no mention of any general guidelines for when to screen and treat for suspected sepsis.
Other jurisdictions have adopted the “Serial Physical Examination” approach, but the details of such an approach vary, it generally requires hourly structured physical examination by a nurse, following a written and agreed protocol, of at-risk infants. This article from Stavanger, Norway, for example, (Vatne A, et al. Reduced Antibiotic Exposure by Serial Physical Examinations in Term Neonates at Risk of Early-onset Sepsis. Pediatr Infect Dis J. 2020;39(5):438-43) is rather vague on which infants qualified as “at-risk”; it seems to be any infants born after chorioamnionitis (undefined) or with a previous sibling with GBS, and “neonates who during the first 72 hours of life developed clinical symptoms indicating a possible sepsis”. All such babies were admitted to the NICU for an hourly structured physical exam.
we accepted mild symptoms (heart rate >160/min, grunting or respiratory rate >60/min, poor feeding and decreased activity) of <2–4 hours duration. We only started antibiotics if these mild symptoms persisted (>2–4 hours) despite corrective actions, if additional alarming symptoms occurred (Table 1) or if the neonate became clinically ill as judged by the attending neonatologist.
This is the Table 1 referred to:
That study was limited to babies of at least 37 weeks, and was able to decrease antibiotic exposure from about 3% to about 1.3%; the incidence of “culture-negative sepsis” also declined dramatically, but remained, supposedly, 50 times more frequent than culture-positive sepsis.
One factor which has probably reduced the incidence of “culture-negative sepsis” is the reduction in CRP measurements! As you will see in part 2, many babies receive prolonged antibiotics to treat their CRPs.
Antibiotic treatment rates much lower than those which follow use of the current EOS calculators can be achieved without any increase in sepsis mortality. Of course the consequences of EOS are not just mortality, untreated, or late-treated EOS may lead to more severe acute illness and long term disability. Such outcomes are very difficult to capture in studies such as these, all-cause mortality is one outcome to be followed, in case babies present with severe illness not recognized as being sepsis, and, in these studies, lower antibiotic use is not associated with increased all-cause mortality.
Decreasing antibiotic exposure in uninfected infants is an issue which is important individually, as it leads to major disturbances of the intestinal microbiome, which are very prolonged, pain caused by IV access, cost, interference with parent-infant interaction, vulnerable child syndrome, and perhaps long term health impacts such as obesity, allergic predisposition, asthma, diabetes, juvenile idiopathic arthritis, celiac and inflammatory bowel disease. To the health care system as a whole, the exposure of a significant proportion of the population to antibiotics must contribute to antibiotic resistance.