I subscribe to Google alerts, which sends me an email whenever the phrase “neonatal research” appears on a new website or a new post. I was interested, therefore to receive an alert about an article which, according the blog “Bioengineer.org”, showed a major genetic contribution to the occurrence of Necrotising Enterocolitis.
The blog post includes the following quote “Bai et al.’s study represents a landmark in neonatal research by providing compelling evidence for the heritability of necrotizing enterocolitis in very preterm infants. The twin study design elegantly disentangles genetic predisposition from environmental influences and firmly establishes a genetic foundation for this complex disease”.
This was intriguing, so I checked on the original article. (Bai R, et al. Genetic susceptibility to necrotizing enterocolitis in very preterm infants: evidence from twin data. Pediatr Res. 2025). A nice study, from a group of authors in China, one of whom is my good friend Shoo Lee, working with the Chinese Neonatal Network. They collected data on NEC incidence and chorionicity of twin pairs of less than 32 weeks GA (or <1500g). They found no difference in the likelihood of a coherent diagnosis of NEC between monochorionic and dichorionic twins. They did further analysis restricting to surgical NEC, or comparing early and late onset NEC, and found no difference between mono- and di-chorionic twins.
In other words, the actual findings of the study are exactly the opposite of what the post on that blog stated. The conclusion of the Bai et al authors was : “heritability does not play a major role in the development of NEC”.
I don’t think an actual human being, reading the article, could possibly have misinterpreted the findings quite as dramatically as whatever generated the blog post. The post is accompanied by the following cute image, which they note was AI generated. My only explanation for this dramatic misinterpretation of the original research article is that the post itself is also AI generated, and that the AI engine just loaded the title and some sub-headings from the results (which are, indeed, misleadingly worded as if there were positive findings : “Heritability contributes to NEC” and “Heritability contributes to certain subgroups of NEC”), without being able to realize that the actual results show that the analysis, of what should have been sub-titled “Heritability contribution to NEC”, was actually zero.
At least this is on an obscure blog, and will probably not cause any harm. In contrast, actual primary publications are also being generated by AI, reporting research that never actually happened. Government policy is also being influenced by review articles written by AI, which include non-existent research, or research which has been misinterpreted, often purposefully so, for partisan ends. This is a major issue for the future of medical research.
Ybarra M, et al. Low-Grade Germinal Matrix Hemorrhage-Intraventricular Hemorrhage and Concomitant Preterm Brain Injuries: Neurodevelopmental Outcomes at 3 Years of Age. J Pediatr. 2025:114713. Previous studies of the long term outcome of infants with germinal matrix or low grade IVH have been inconsistent. Some have shown an association with poorer developmental progress, and others have shown no impact. Some of this variability may be due to uncertainty about diagnostic criteria, with slightly larger amounts of intraventricular blood being classified differently. Some is probably due to the variable association with other brain injury, not readily seen on ultrasound, such as white matter injury, or cerebellar haemorrhages. We now routinely perform imaging of the posterior fossa, which was not easy with older ultrasound machines, but small cerebellar haemorrhages are still hard to see, without MRI.
In this cohort from Toronto, 175 infants <32 weeks GA had ultrasounds, they also had early cerebral MRI at 32 to 34 weeks, if they were stable, and then again at term equivalent age. Neurologic and developmental assessments were performed at 3 years (Bayley version III). As for the results, low grade haemorrhages had no correlation with outcomes, unless associated with either large cerebellar haemorrhages or more extensive white matter injury. It has always been fascinating to me that germinal matrix haemorrhage, which destroys the primary source of cortical neurones, has so little impact on long term outcomes. It speaks to the plasticity of the newborn brain, if the Germinal Matrix is injured, other parts of the brain take over neurone production.
Take home message : there was no apparent impact of GMH or small intraventricular haemorrhages without dilatation on long term development. Cerebellar haemorrhages, if large, are associated with delayed language development at 3 years, and white matter abnormalities, if extensive, are associated with motor delay, and cerebral palsy.
Interesting review article on the impact of pasteurization, using the standard (Holder) pasteurization method, as well as some information about alternatives. The dash (-) in the figure above means no effect, rather than deletion. As you can see there are multiple impacts of pasteurization, as well as the expected impact on bacteria, some bacteria are resistant to Holder pasteurization, so donor breast milk still has an impact on the preterm intestinal microbiome. Both by direct colonization with the surviving organisms, but also because of the impact of HMOs and other components of human milk which remain despite pasteurization.
The figure also shows, in the upper right third, some alternative pasteurization methods which have been investigated, and which all show lesser impacts on breast milk components, HTST (high temperature short treatment) HPP (high pressure pasteurization) and UV-C (UV-C!). These alternative methods are equally effective at reducing bacterial load in the donor milk, and hopefully can be used in the future to give donor milk which is closer to Mothers Own Milk.
Take home message : Holder Pasteurization has major impacts on the composition of human milk. Alternative methods should be investigated, and approved.
In this observational study, the authors correlated the diet of a cohort of preterm infants <32 weeks GA with the findings on MRI at term. The cohort was enrolled over a long period, including a couple of years prior to the availability in their centre of donor milk (DHM) 2012-2014, and several years afterward 2014-2022. They include babies who almost exclusively received Mother’s own milk (MoM) and those receiving mostly formula, as well as the group with DHM. Brain volumes were greater in the human milk groups compared to formula, and diffusion tensor imaging showed diffusivity differences also, in the Corpus Callosum and the PLIC (posterior limb of the internal capsule). As the authors note, there is no good evidence from RCTs that DHM leads to better clinical neurological or developmental outcomes than formula. Nevertheless, these data are consistent with a beneficial effect of human milk on brain development, shared by DHM, and MoM.
Take home message : human milk seems to promote larger brains.
One of the benefits of MoM is that it routinely contains probiotic organisms, usually including Bifidobacteria. In this trial, 70 preterm infants <32 weeks were randomized to control or to a supplement of Bifidobacterium animalis susp lactis. As often happens in some journals the article is written in somewhat strange English; one example : “Quality control and data analysis were conducted after instrument analysis, using assessment of the peak significante equation of standard curves”. They ran a statistical comparison of the baseline characteristics of the randomized groups. This is a practice that Pediatric Research should know is ridiculous. If the groups were randomized, why run such a statistical test? It is superfluous, potentially misleading, and the CONSORT statement specifically states that it should not be done, Pediatric Research is supposed to follow CONSORT guidelines.
I started to include this article in the post as I thought it was a demonstration of the possible anti-inflammatory impact of this Bifidobacterium on the preterm intestine. But I now realize that I haven’t got a clue what most of it means. This following figure for example, is supposed to show correlations between a large number of “metabolites”; about 30 were selected from over 250 that were found in the stools, including, for example, 34 different bile acids. These figures are supposed to show correlations, negative and positive, between “metabolites”.
The legend to the figure states “Red indicates positive correlation, blue indicates negative correlation, and the darker the colour, the stronger the correlation. a Probiotic group week 2 VS Control group week 2. b Probiotic group week 2 VS Control group week 2″…. What on earth is this supposed to mean? Aside from the fact that the potential of at least 62,500 comparisons were possible, is this comparison within the 2 groups, or between the 2 groups?
What it seems to show is that they measured a huge number of molecules, the concentrations of some of them were correlated with the concentrations of others. But so what?
They also show dramatic differences in serum TLR4 concentrations between groups. I am unsure if circulating concentrations of TLR4 are of any interest; TLR4 is normally attached to granulocytes, as part of the receptor complex which recognizes lipopolysaccharide. Nevertheless, published serum concentrations range between the pg/mL range to the mg/mL range, with these new results being intermediate in the ng/mL range. Such enormously variant normal ranges (over 1 million fold differences) make me very sceptical about any results. Serum TNF-α and IL-Iß were also dramatically lower in the Bifido group. They also give exactly the same data, regarding clinical complications, in table 3 and a completely superfluous figure 10.
Pediatric Research used to be a journal that only published high-quality research, although they were rarely clinical studies, which was previously one of my criticisms of the journal. If this is typical of the quality of what is currently getting through peer review and editorial control, then the journal has fallen far indeed.
Take home message : Pediatric Research is no longer the high-quality source it once was.
This is a report of the 3 year outcomes of babies from a cluster RCT of a quality control initiative in Japan. The original publication showed no impact of the QI program (INTACT), so the authors combined the groups for this publication describing their neurological and developmental outcomes. Babies were VLBW and ranged from 22 to 31 weeks GA. Below is a selection from the extensive results, “severely delayed” refers to being <70 on the cognitive subscale of the Kyoto Scales of Psychological Development. The KSPD seems to have a similar mean to the BSID ver3, when tested on the same infants, but have a wider distribution, so a score <70 was considered severely delayed.
There was very little blindness or deafness, so, as usual, it was cognitive delay which was responsible for most of the infants who were classified as “NDI”. Unfortunately, the authors don’t report many things which matter to parents, in particular there is no mention of behavioural problems. They do have a table that they call “functional outcomes” but that is actually a report of the medical interventions being received by the infants, at 3 years of age, including home oxygen, NG tube feeding, anticonvulsant medications, etc. All of which were rare.
Take home message : The majority of survivors at every gestational age, even the most immature, do not have “moderate or severe NDI”. There is a progressive increase in “moderate or severe NDI” as GA decreases.
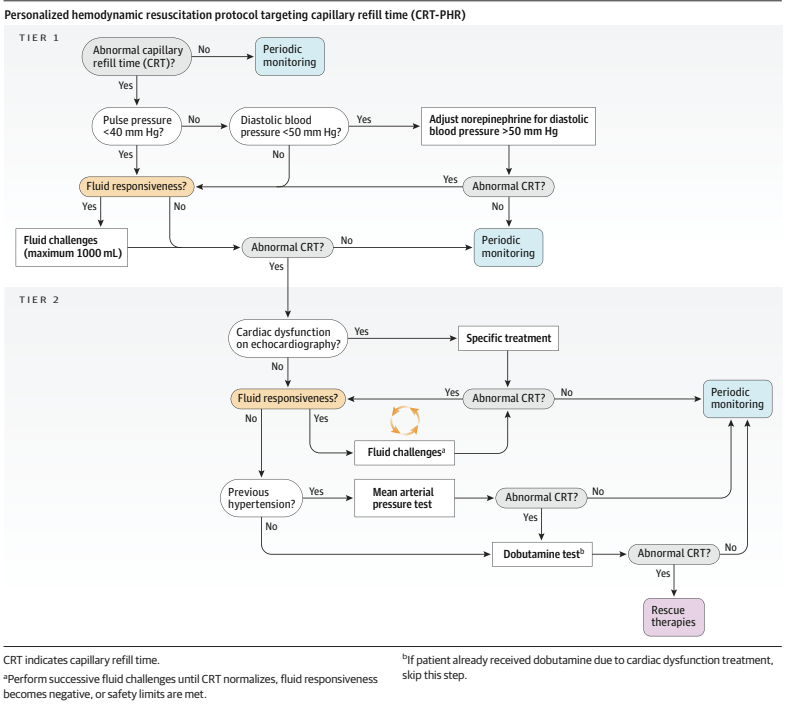
This is a very interesting trial evaluating the usefulness of clinical assessment of the circulation in adults with septic shock in a large international multicentre trial. Patients with suspected sepsis, who required norepinephrine after 1 litre fluid bolus, and had an elevated serum lactate, were randomized. A standardized method of measuring capillary refill time was agreed upon,
CRT was assessed by applying firm pressure to the ventral surface of the distal phalanx of a finger, using a glass microscope slide. The pressure was increased until the skin was blank, maintained for 10 seconds, and then released. The time required to return to the normal skin color was measured with a chronometer and a refill time longer than 3 seconds was defined as abnormal
and the algorithms were activated if the cap filling time was abnormal in the CRT-PHR (cap refill time- personalized haemodynamic resuscitation) group.
As you can see, if the CRT was >3 seconds, you first check the pulse pressure, and if it is >40 mmHg, then you check the diastolic BP, which may lead to increasing norepinephrine dose; the next stage may be to give more fluid to see if there is a response, and then progress to bedside echocardiography, which may lead to specific treatments, or more fluid, or eventually to low dose dobutamine.
The control group had “standard care”, CRT was recorded but the algorithm was not followed.
The primary outcome was a hierarchical composite: (1) all-cause mortality within 28 days, (2) duration of vital support (vasoactives, mechanical ventilation, and kidney replacement therapy) truncated at day 28, and (3) length of hospital stay truncated at day 28.
The trial was analyzed by the Win Ratio. 1400 patients were randomized, as it was not a paired study (one way of using the Win Ratio), but individually randomized, they stratified the patients by APACHE score, then, within strata, every patient in group 1 was compared with every patient in group 2, to determine if they won or lost. There were therefore 244 000 paired comparisons. The CRT-PHR group won 49% of the comparisons, compared to 42% of the control, usual care group. The remaining 9% were exact ties.
This exceeded the limits for statistical significance; mortality was identical at 26.5%, but there were more ICU free days, and shorter hospital stays in the CRT group. The table of interventions shows that more of the CRT group received vasopressin, more received dobutamine, and they received less fluid; at 6 hours of treatment, their CRT was shorter, and serum lactate was lower.
The analysis is illustrated below in the 2 strata of the Apache Score (a higher score predicting higher mortality); this showed a greater difference in the sicker patients.
I found this fascinating. In terms of the intervention being investigated, trial design, and analysis methodology.
Many of my readers will know of my concerns about the way we analyse composite outcomes in neonatology. Comparing “death or BPD”, “death or NDI”, “death or hiccups”, between randomized groups, as if they were of equal importance, and as if we were always sure that they would change in the same direction with an intervention. This trial is one of a growing trend to using hierarchical composites, with death being given the greatest weight in the analysis, followed by other clinical outcomes in descending order of importance. Clearly an example to be followed in neonatology.
Combining such clinical signs with the direction of change in serum lactate (the absolute value doesn’t help much in the first couple of days as it is often high after birth), urine output (also not much use immediately after birth), level of activity etc, seems to me to be likely to be important in determining treatment in septic babies also. But we have very few good randomized trials of treatment approaches in septic newborns.
This trial gives us some pointers of how we could reasonably design such a trial, with a structured algorithm of interventions, including clinical pointers and targeted functional echocardiography in some patients, and how to design and analyse the primary outcome. We could develop a consensus algorithm (it couldn’t really be evidence-based) and test against usual care, with a hierarchical composite outcome including death and brain injury and duration of intensive care support, for example.
Unfortunately all of the large confirmatory studies have been completely null, without a hint of a benefit. Including LIFT-Canada, which is in submission so I won’t go into any details, but I can say that we did not show a benefit of bLF.
There continue to be some trials which do seem to show an effect of bLF, including this very new trial (Plaza-Astasio V, et al. Preventing Sepsis in Preterm Infants with Bovine Lactoferrin: A Randomized Trial Exploring Immune and Antioxidant Effects. Nutrients. 2025;17(19)). Just over 100 VLBW infants were randomized to bLF supplementation or control, prior to 72 hours of age, and followed for LOS, as well as lab tests of antioxidant and immunologic effects. LOS was defined as “Laboratory confirmed sepsis” after 72 hours. The authors followed the NeoKisses definitions, which, as far as I can tell, include so-called “clinical sepsis” without a positive blood culture, but in the supplementary materials of this new study there are the same number of organisms listed as the episodes of sepsis, that is 11 in the bLF group and 21 in the placebo group. In other words they showed a reduction in culture-positive sepsis.
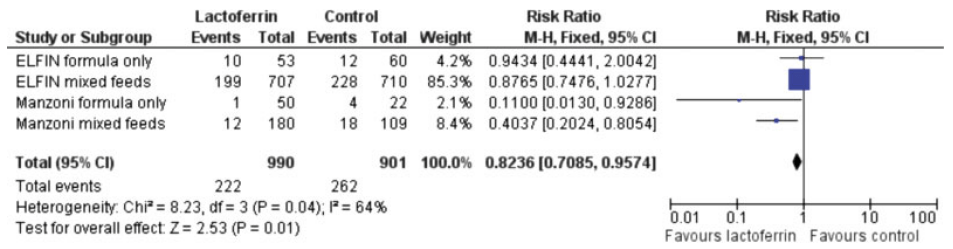
The authors note that their breast feeding rates were lower than some of the other large trials, at around 75% compared to over 90% in the large trials, and suggest this as a possible explanation for the difference of their results compared to the larger RCTs. That seems to me doubtful, if bLF was only effective in formula fed babies, then they could not have shown such a large decrease. Ochoa and her collaborators have published an IPD meta-analysis of the VLBW infants enrolled in their 2 trials (see below) which suggested that the impact of bLF was much greater among babies with low human milk intake (11% bLF, 21% controls). Although they do indeed show that, what is strange is that their analysis shows that LOS was much more frequent in babies with a high human milk intake, either with bLF (35%) or in their controls (39%), which is hard to understand. Another secondary analysis, of the data from ELFIN and the original Manzoni trial, showed similar reductions in LOS by bLF among breast-milk fed and formula fed, or mixed feeds babies. The reductions in LOS by bLF were very small and consistent with random variation in ELFIN. The interaction term was not significant, suggesting that the reduction in LOS was similar regardless of feed type.
The authors of the new study also note that their control frequency of sepsis was high, which is again true, a 40% incidence of LOS in a group of infants with a mean GA of 30 wks is extremely high. Having a higher baseline frequency of an abnormality will generally tend to make the impact of an intervention seem greater (see my recent posts on regression to the mean), but that doesn’t mean that such an impact would disappear completely when the incidence is lower.
One other difference that they do not mention is the source of bLF; the newly published trial used DicoPharm, just as did Manzoni. Akin’s study used the same product and also showed a reduction in culture-positive sepsis. Theresa Ochoa in her 2 studies used a product from Tatua ™ in the first study, derived from pasteurized milk, which had no effect on culture-positive sepsis, and a product from Friesland Campina in the other trial, which seems to be extracted by freeze-drying and not heat treated. The second trial showed a decrease in culture positive sepsis (from 11 to 8%, NS) not shared by the first study. Other studies either don’t mention the source of the bLF (Kaur et al) or I cannot obtain them as they aren’t in PubMed, or any other database that I can access (Liu, Tang, Dai). Another new study, from Egypt, randomized only formula fed infants (Ellakkany N, et al. Influence of bovine lactoferrin on feeding intolerance and intestinal permeability in preterm infants: a randomized controlled trial. Eur J Pediatr. 2024;184(1):30). They had an enormously high rate of LOS in the controls (60%) and a lower, but still extremely high, incidence in the bLF treated infants, 43.3%. The preparation they used was produced in Egypt, and I can’t find any details of how it was prepared. Finally I found one other trial, performed in Pakistan in infants with an average GA of about 34 weeks, (Ariff S, et al. Evaluation of Bovine Lactoferrin for Prevention of Late-Onset Sepsis in Low-Birth-Weight Infants: A Double-Blind Randomized Controlled Trial. Nutrients. 2025;17(11)). with a product from Hilmar in the USA which appears to have been prepared from freeze-dried milk (and perhaps not heat treated), they had an 8% incidence of culture-positive LOS in controls, and a combined 6% in the 2 treatment groups (with 2 different doses of bLF); total n of about 300.
There are lab studies showing that pasteurization decreases the biologic activity of bLF. bLF is degraded by heat treatment, it aggregates, and bind iron less well (Remadevi R, Mead D. A Study on the Bioavailability of Lactoferrin under Pasteurisation at Different Conductivities and Solid Contents. Journal of Food Research. 2025;14(2)). It could well be that heat-treatment of milk, prior to extraction of bLF, causes sufficient structural changes in the molecule for it to no longer have the multiple beneficial effects on bacterial proliferation that have been documented. This might be one reason why donor human milk (which is always pasteurized, usually by Holder pasteurization, the only method approved by HMBANA) is less effective at decreasing NEC than Mothers own Milk.
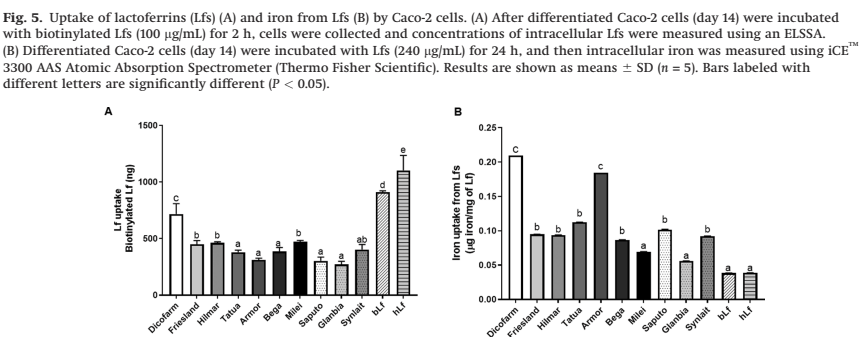
There are, however, known to be major differences in the biologic activity of different sources of bLF. One study examined 10 different bLF sources, and compared several different aspects of structure and activity between them, as well as their own bLF and human LF (Lonnerdal B, et al. Biological activities of commercial bovine lactoferrin sources. Biochem Cell Biol. 2021;99(1):35–46). There were major differences between bLF sources. As one example, they examined uptake of the LF by Caco-2 cells, and whether the LF transported iron into those cells
The details of what that means are not that important here (partly because my own understanding is limited, but also because it isn’t certain what this particular aspect has to do with their biologic effect of decreasing infections), but what this does show is that different sources of bLF are extremely different. They also found very variable degrees of contamination of the bLF product with other proteins, the Hilmar product, as one example “contains a relatively low concentration of Lf and relatively high concentrations of a-S1-casein, a-S2-casein, and J domain- containing protein”, whereas the Dicopharm product had lots of LF and relatively less of the other proteins.
I think, before we give up completely on bLF supplementation as a potential way to decrease LOS in the preterm, there is room for another study, investigating specifically the Dicopharm product, which has been consistently associated with decreases in culture-positive LOS. It may be that the story of bLF to prevent LOS still has a twist in the tale.
After my post on regression to the mean, and its importance in studies of apnoea therapy, I was thinking of other examples. Some which have been most evident to me are those which impact on areas of medicine that I have researched myself. One example, from many years ago now, looked at the haemodynamic effects of dopamine in sick preterm infants. Seri I, et al. Regional hemodynamic effects of dopamine in the sick preterm neonate. J Pediatr. 1998;133(6):728–34.
This study was performed during the 1st 2 days of life, a period when blood pressure normally gradually increases, and when renal vascular resistance falls dramatically. These known baseline changes are an additional confounder in the results of non-controlled studies. The subjects were preterm infants with what they termed “compensated shock”, that is they had a BP between the 10th and 90th percentiles, but were oliguric (<0.6 ml/kg/h of urine) and/or had slow capillary filling. They were all given dopamine, with echographic indices performed before and after.
What you can see is that overall mean BP increased, after doses of dopamine between 2.5 and 7.5 microg/kg/min
And an index of renal vascular resistance, the pulsatility index in the renal artery, decreased
These are actually changes that you would expect over time in the first hours of life. The time difference between the 2 measurement was relatively short, at about 30 minutes, one could argue, perhaps, that the changes are too quick to just be postnatal adjustment. Maybe they were caused by the dopamine?
Interestingly, the authors also presented results after, post hoc, dividing the infants into responders (who had a >10% increase in mean BP) and non-responders.
This shows that, the “responders”, panel A, had a lower mean BP before dopamine treatment, of about 35, and it increased to about 43 afterwards. The “non-responders”, panel D, had a mean BP, before and after dopamine, of just over 40 mmHg.
This is exactly what you would see if the results are entirely due to regression to the mean. Those with lower BP than average will tend to have an increase after any treatment, including placebo. It would be surprising, in an observational study such as this, for them to have given dopamine to babies with a higher BP than average.
Having said that, dopamine will in some circumstances, I think it is clear, increase BP, probably not by much at a dose of 2.5, but there is enormous variability in dopamine kinetics (and pharmacodynamics); some infants might have an increase in BP at low doses, and some have no effect at very high doses. Dopamine is, however, an effective vasoconstrictor, and any increase in BP is entirely due to vasoconstrition in the newborn. In this study, however, both “responders” and “non-responders” had a decrease in renal vascular resistance, why would this be? As I mentioned above, renal vascular resistance is known to decrease dramatically after birth; this study, for example shows an 88% decrease in RVR over the first 2 weeks of life, most of which is in the first 2 to 3 days.
I also subjected the animals to an infusion of Fenoldopam, as selective agonist of vascular dopamine receptors, which showed absolutely no renal vasodilatation.
These examples demonstrate, yet again, that one has to be very sceptical about the results of observational studies of the responses to an intervention. Whenever we treat a baby who has a problem which varies in intensity, be it apnoea, low blood pressure, oxygen requirements, oliguria, or anything else that you can think of, unless you randomize and treat only half of the infants, one can never know if any changes which are seen are due to the intervention, or just regression to the mean. Babies with BP lower than average will always tend to have higher BP the next time you measure it. Babies with low urine output will always tend to have higher urine output after an interval.
Controls, controls, controls. Preferably randomized controls. They are essential for determining the impacts, efficacy and safety of our interventions.
I mentioned in my previous post, an issue with meta-analyses; there have been several I have read recently which are very problematic. They seem to be produced by groups that have little concern for the quality of their product.
This article is free access, which means that someone paid about $4600 US to put this misleading nonsense on line. Springer journals commonly publish poor quality articles under their pay-to-publish model, and really, if any peer reviewer worth his salt had read this, it is immediately evident that there are huge issues. Just to take one other minor example, they state that the ETTNO trial did not describe the means of randomization, I guess the SR authors just didn’t read the methods which actually describes them in more than the usual detail : “The random sequence was computer generated with variable block size (2-10) using the software RandList version 2.1 (DatInf)”.
They also have weighted some outcomes in a way that the small, unobtainable Chinese trials (n of between 70 and 180) have much more weight in the analysis of duration of oxygen (for example) than the large ETTNO trial (n>1000). This is presumably because of the minuscule SD of the data from those trials, for example Wang 2013 apparently showed a duration of oxygen in the liberal transfusion group of 14 days (SD2) compared to 18 days (SD3). This study of 86 babies has a 40% weight in the analysis as a result, compared to ETTNO, given an 11% weight, probably because the SD of the duration of oxygen therapy is realistic, 50 days (SD33). My guess is that the supposed SD of duration of O2 therapy in Wang, and the other trials with extremely narrow distributions, is actually an SEM, but as the articles are inaccessible there is on way to check that.
To explain further, continuous outcomes in meta-analyses are usually weighted by the inverse of the variance. This is done so that articles with more precision in their estimates (usually the larger trials) have more impact on the calculated overall mean effect. When the variance (however it is reported) is very small, then the article might have an outsized impact on the MA, which is why it is so important to be sure that the data are reliable, and that the reported variability in the data is really a SD, and not a SEM.
If the analyses were redone, giving appropriate weight to the larger trials, then there would be no impact of transfusion threshold on respiratory outcomes.
This matters. Individual carers could give transfusions to preterm infants with the expectation that they will shorten the duration of oxygen therapy, or positive pressure respiratory support, based on this erroneous SR/meta-analysis.
Recently, when I do a lit search, I often find more Systematic Reviews and Meta-Analyses that there are original trials. I think there are academics who think its so much easier to just recycle the results of someone else’s research than to perform a trial themselves.
Reputable journals should be very careful about publishing SR/MA. They should ensure that the SR was registered, and follows PRISMA guidelines and ensure that they are not just re-performing reviews that have already been well done. They should require that the authors provide pdf copies of the original trial publications with the submission, so that peer reviewers can verify the accuracy of what is being presented. Peer reviewers should ensure that the articles included really exist, that they are trials of the intervention being evaluated, and that the results are accurately analysed.
A related issue is the question of whether the original data are reliable or not. I have read, and reviewed, articles which seem to have been written by AI, and which are probably entirely fictitious. Others have probably skewed their results to be more positive, or have reported different outcomes to those planned when they found something interesting post hoc. A new tool has been developed to try and counter these issues, called INSPECT-SR, which is available as a preprint. (Wilkinson J, et al. INSPECT-SR: a tool for assessing trustworthiness of randomised controlled trials. medRxiv. 2025:2025.09.03.25334905). The tool gives multiple checks to perform when writing an SR, as an attempt to eliminate data which are not reliable. It is a very sad that the integrity of published trials has to be questioned, but it is a reality of our current state of affairs.
Determining the integrity of a Systematic review is even more difficult, as one often does not have access to the original trials, to see if they have been accurately interpreted. The 2 SRs that I have recently criticized, one about Caffeine in the newborn, and this one about transfusions, are both addressing issues for which I was an author of one of the major included trials. My involvement made it immediately obvious to me that there were serious errors in interpretation, and that the SR/MA was very flawed. Systematic reviews of other issues, that I have had less direct involvement with, may have been just as flawed, but it could have escaped my notice.
There is much pressure in some academic circles to “publish or perish”, and to get something, anything, in to print. In some countries medical students are expected to publish an article prior to being awarded their MD degree. In others, junior academics cannot advance unless the combined weight of their output,when printed, exceeds a certain number of kg (or at least it seems that way). Journals now have a major interest in publishing anything that is submitted along with a cheque. Springer seem to be particularly egregious among the older established publishers, but some newer groups, like the Frontiers journals and MDPI have an extremely uneven profile, some of their titles being clearly predatory pay-to-publish journals, and others having higher standards.
It is incumbent on us, in the present day, to be sceptical of everything that we read, primary research and SRs. Pre-registration of trials and SRs, and data sharing are essential to ensure the integrity of the research on which we base our clinical decisions for critically sick babies.
There has for a long time been a thought that anemic babies with many apnoeas could benefit from a blood transfusion which would decrease their apnoeic spells. This idea has never been directly tested by an RCT. That is, a trial in which infants with apnoea were randomized to receive a transfusion or control, and the response accurately determined. I actually started such a trial when I was in San Diego, but only enrolled a tiny number of babies before leaving to return to Canada; the fellow who was involved finished at about the same time as me, and the project was sadly terminated. I admit that it is not ethical to randomize infants to a trial, with all the stress imposed, and the goodwill of parents involved, and then not have a mechanism to complete the trial, and I apologize to the parents and families involved.
The evidence we do have, therefore, comes from observational studies of various kinds and from secondary analysis of RCTs of blood transfusions at differing thresholds, in which the impacts on apnoea or on intermittent hypoxia (IH) have been recorded. Just to remind my readers, most IH is caused by apnoea, prolonged recordings of saturation are much easier than the prolonged multichannel recordings required to objectively quantify apnoea. I will use the terms interchangeably here, partly because the harms of multiple recurrent apnoea spells, are probably because of frequent desaturation leading to hypoxic injury, and resaturation, with consequent oxidative injury.
Interestingly, the 2 types of evidence give contradictory results. Observational studies tend to show a reduction in apnoea, or IH, after a transfusion, whereas RCTs don’t show a difference in apnoea, or IH, by randomized group; those with a haemoglobin maintained at a higher level do not have less apnoea/IH than those allowed to have lower Hgb.
This is an object lesson in the hazards of observational studies, especially for a condition which is very variable in severity (between patients and between days) and which eventually improves.
I actually use this example when I teach statistics and research design to fellows!
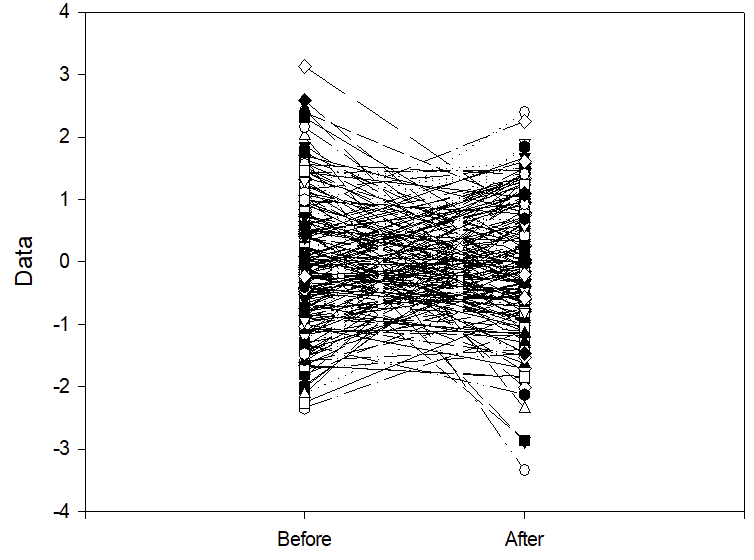
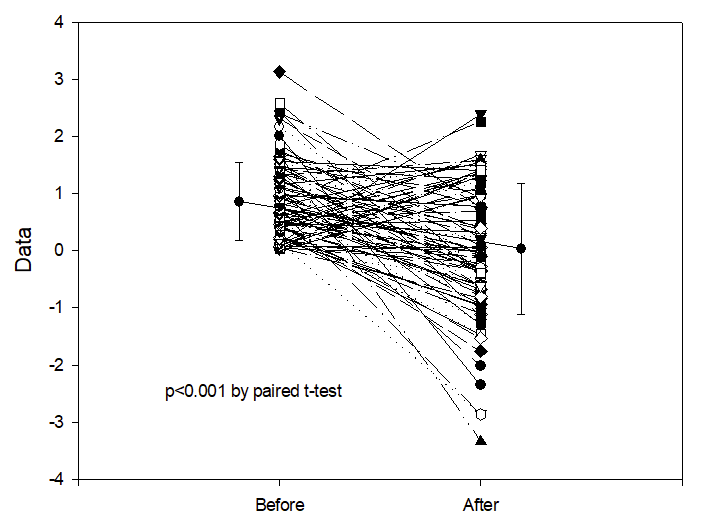
The figure below shows two columns of randomly distributed numbers which I generated, each connected by row number, with a mean of 0 and a SD of 1. If we take “0” to mean the overall average frequency of IH per hour in the sample, (it could be 4, for example), the numbers on the vertical axis are the number of Standard Deviations above and below the mean, this figure could be the number of IH per hour on day 7 and on day 14 of life of 200 preterm babies.
If one decides to give a treatment only to those babies who have more IH than the mean, which means you are selecting the babies in the top half of the distribution, then measure IH frequency again after the treatment. Then, even if the treatment had no effect whatsoever on IH frequency, the result you would get is shown below.
This is regression to the mean. There are very many examples of this, as a potential explanation of positive results in observational studies. Let me give you one example, of an uncontrolled study of of an apnoea treatment. Marlier L, et al. Olfactory Stimulation Prevents Apnea in Premature Newborns. Pediatrics. 2005;115(1):83–8. In this study, babies having recurrent apnoea were exposed to a nice smell, lavender wafted through their incubator, and they evaluated apnoea frequency afterwards. There were fewer apnoeas when the babies had a pleasant odour in the incubator! Without a randomized control group such data are worthless. Any variable condition will tend to get better if you start treating it when it is worse than average, whether you use something effective or give a placebo.
If you tend to give transfusions to anaemic babies who are having more apnoeas, then you are immediately creating exactly this situation. If transfusions have no impact on apnoea, then an observational study will show a significant reduction in apnoea frequency following transfusion.
Also striking is what happens if you ask the question, “do babies who have the most apnoeas have the greatest benefit from transfusion?”, then plot the initial apnoea frequency against the improvement after the treatment, using the randomly generated numbers in the figure above, this gives a correlation coefficient of 0.56 and a p-value of <0.0001.
Remember, these are from entirely random numbers, after an intervention with no real impact whatsoever on apnoea frequency! All you have to do is select the most severely affected babies to treat, they will seem to improve the most.
IH decreased from 5.3/h to 3.6/h after blood transfusion, and was unchanged at 4.6/h before and after the small number of transfusions of other blood products.
This is exactly the result you would expect if caregivers were more likely to transfuse anaemic preterm infants when they were having a greater than average number of IH, but give plasma, platelet, or other transfusions for reasons that have nothing to do with apnoea; even if there were absolutely no effect of transfusions on apnoea incidence or IH.
I am not picking this study out as a particularly egregious example, in fact, it is a better study than most, as it at least had the non-RBC controls. You would also see something similar if there was a real impact of RBC transfusions on IH.
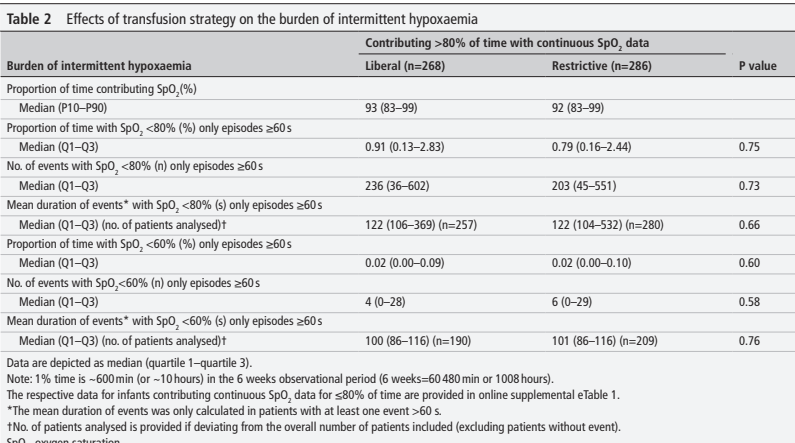
If we look at the RCTs of blood transfusions in the preterm, which have compared different transfusion thresholds, there is no apparent impact on IH or on apnoea. This includes the most recent publication, which is a secondary analysis of an RCT. (Franz AR, et al. Effects of liberal versus restrictive transfusion strategies on intermittent hypoxaemia in extremely low birthweight infants: secondary analyses of the ETTNO randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2025). The ETTNO trial was a randomized comparison of differing transfusion thresholds in infants <1000g birthweight that I have already discussed, which showed no impact on the primary outcome of “survival without NDI”. There was no impact in survival or on developmental progress, as measured by the Bayley version 2 MDI, results of which were identical between groups. The transfusion thresholds were a bit complicated in ETTNO, the high threshold group had 3 different thresholds according to postnatal age in stable babies, and 3 higher thresholds in “critically ill” babies. The low transfusion group had a different matrix of 6 transfusion thresholds according to postnatal age and being stable or not. Of note, one of the indications for being considered “critically ill” were 6 or more apnoeas/day requiring nursing intervention, or IH to <60% saturation >4 times per day.
This new secondary analysis compared IH frequency and severity according to randomized group. About 50% of the babies had good enough recordings of saturation for analysis, a subgroup who seemed representative of the whole sample.
There were no differences in any index of IH between groups.
In the PINT study, one of our secondary outcomes was how many babies in the low vs high transfusion threshold transfusion groups had “apnea requiring treatment”, which was 55% in the lower Hgb group and 60% in the higher Hgb group, in other words, the small difference was in the opposite direction and not in favour of an impact of Hgb on apnoea frequency.
I don’t think there are any secondary outcome data on apnoea or IH from the TOP trial, if anyone knows of any, please let me know. A much older trial (1984) of only 56 preterm infants reported apnoea frequency among infants randomized to either have their Hgb kept above 100 g/l, or to be transfused only for clinical indications, including surgery, but also including severe apnoea not responding to theophylline as a clinical indication. There were no differences in recorded apnoea frequency despite differing Hgb concentrations. The only controlled data which show a possible impact on apnoea are from the Iowa trial, of 100 preterm infants <1300 g (Bell EF, et al. Randomized trial of liberal versus restrictive guidelines for red blood cell transfusion in preterm infants. Pediatrics. 2005;115(6):1685–91) which had more apnoea spells in the lower threshold group, and more apnoea requiring nursing intervention, 0.4/day compared to 0.2/day. In that trial, infants were allowed to receive a transfusion, even if they were in the low threshold group, if they had multiple apnoeas, which is a possible confounder in analysing the meaning of that result.
I looked for systematic reviews of transfusion in the preterm to see if any had analysed the impact on apnoea, and was unable to find any other reliable data, but read my next post to see what I did find.
My take home message is that there are few reliable data to show that apnoea or IH is more frequent in infants with lower Hgb, nor any reliable evidence that RBC transfusion reduces apnoea or IH in the preterm.
If you transfuse babies who are having more apnoea, or more IH, than average they will usually have a reduction in their episodes.
But :
If you don’t transfuse babies who are having more apnoea, or more IH, than average they will usually have a reduction in their episodes.
The only way to resolve the issue would be to do a trial similar to the one that I started years ago. Enrol anaemic infants with apnoea or IH, randomize them to transfusion or control and obtain objective recordings of their responses. I have a strong feeling, based on my evaluation of the currently available data, that both groups will show a reduction in apnoea/IH, and that there would be little or no difference between the two groups.
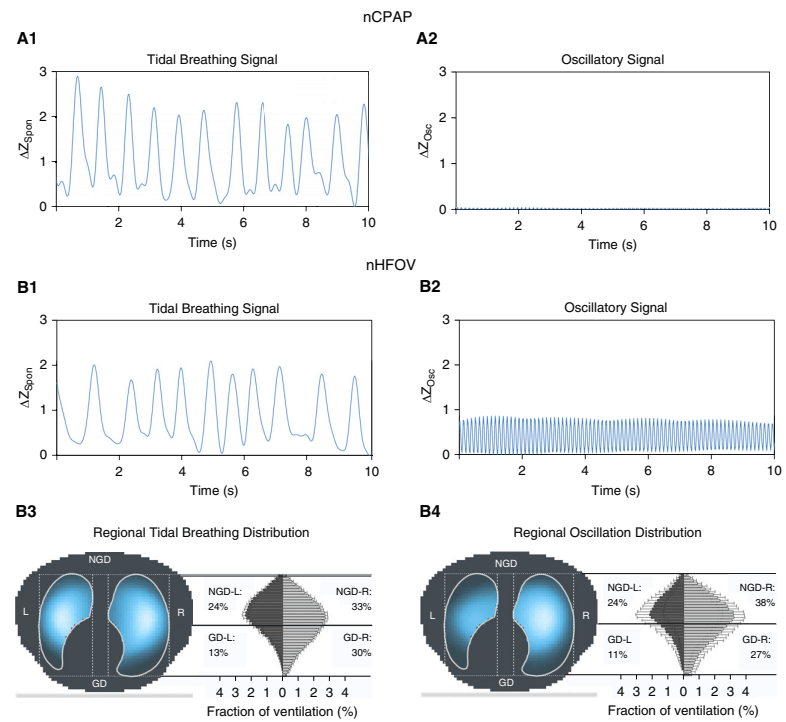
Non-invasive HFOV can be delivered by a variety of different equipment and interfaces. The high flows and upper airway turbulence probably have an impact on gas exchange; It appears that the effective dead space of the oro-nasopharynx is washed out (De Luca D, Dell’Orto V. Non-invasive high-frequency oscillatory ventilation in neonates: review of physiology, biology and clinical data. Arch Dis Child Fetal Neonatal Ed. 2016;101(6):F565–F70), but how much transmission of the oscillatory pressures to the lung occurs is uncertain. Transmission does occur under some circumstances, however, as several groups have shown. In this cross-over study, for example, (Gaertner VD, et al. Transmission of Oscillatory Volumes into the Preterm Lung during Noninvasive High-Frequency Ventilation. Am J Respir Crit Care Med. 2021;203(8):998–1005) nHFOV was applied starting with a pressure amplitude of 20 cmH2O, then adjusted to give either a PCO2 of 40-60, or, if, the baby was already normocapnic, adjusted to the lowest pressure that gave visible chest wall oscillations, the article doesn’t state what were the eventual pressure amplitudes received. Nevertheless, using transthoracic impedance tomography, they were able to detect chest wall movements which were about 1/5 the amplitude of the babies tidal volume movements. They also showed that when the oscillations were switched on, there was a decrease in the amplitude of the infant’s own tidal respiratory movements, which I presume was a reflex reduction, secondary to an increase in CO2 clearance by the HFO, which would decrease endogenous respiratory drive.
The figure shows the amplitudes of impedance changes over a period of CPAP compared to nHFOV, i the upper panels, and the lower coloured pictures show that the oscillations were preferentially transmitted to the right lung, especially the central and “upper” regions (the babies were in ventral positioning).
It appears likely, then, that there are some pressure oscillations in the distal airways during nHFOV, which might lead to some gas exchange. It is possible, therefore that respiratory support of nHFOV may have some advantage over CPAP. Any possible advantage over nIPPV (with NAVA or fixed pressures and/or non-synchronised) is not so clear, and requires some clinical trials to confirm.
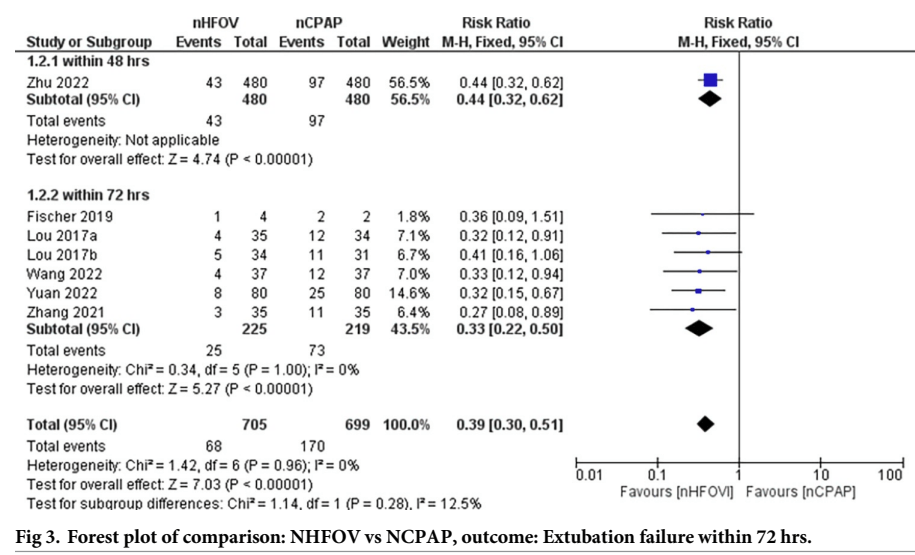
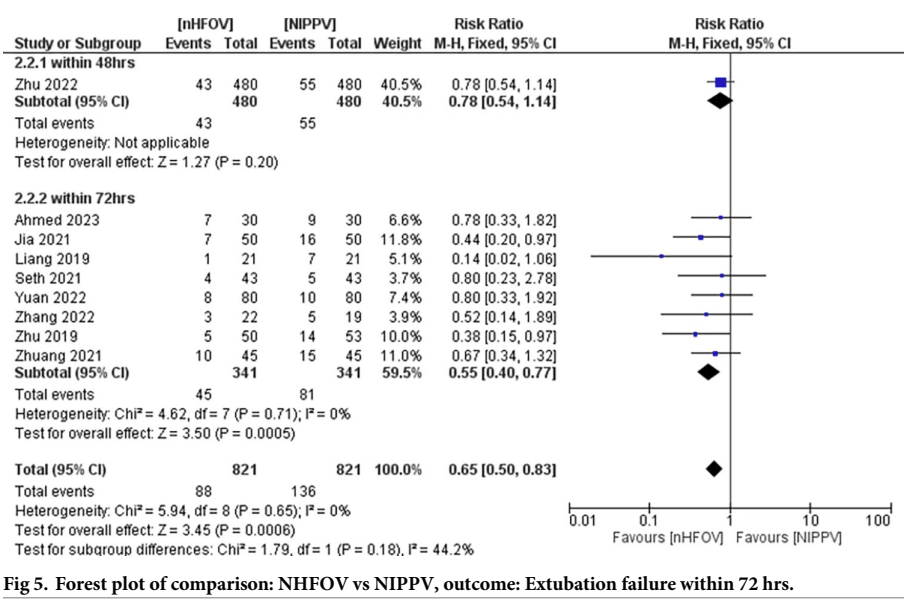
There have been a few recent trials of nHFOV, both as a mode of routine support post-extubation, and for primary respiratory support after birth in preterm infants. There are also now several systematic reviews and meta-analyses, there seem to be some SR/MA factories churning these things out, some of which appear to have been written with AI, and sometimes include non-existent references. One needs to be really careful these days, both as a reader and as a peer-reviewer. I now check much more carefully than in the past when I am peer-reviewing an article (both primary research and review articles) to be sure that the key references actually exist. Unfortunately I don’t read Chinese, and many references only seem to appear in Chinese databases. In this SR of post-extubation nHFOV, for example, Prasad R, et al. Noninvasive high-frequency oscillation ventilation as post- extubation respiratory support in neonates: Systematic review and meta-analysis. PLoS One. 2024;19(7):e0307903 there are numerous included RCTs for which I cannot find the original article, some appear to only show up when searching the Chinese medical publication database, so it is impossible for me to check the definitions of treatment failure, for example, or the characteristics of included babies.
That review shows a reduction in extubation failure when nHOV was compared to nCPAP
and a smaller advantage of nHOV compared to nIPPV
That review showed no difference in any other clinically important outcomes, such as lung injury as measured by BPD at 36 weeks, IVH, or the other usual neonatal complications. It also is not clear if all the babies benefited from an optimal approach to extubation, with caffeine pre-treatment, evaluation of spontaneous breathing, and higher CPAP levels in those still requiring oxygen, all of which can reduce extubation failure rates, and might eliminate a possible advantage of nHFOV, or not. They are also all tiny or modestly sized trials, only one of which was individually significant, which inflates the probability of a chance finding.
In addition, as mentioned, there are some problems with availability of these publications. The reference list of this SR/MA has no entry for Zhu 2019, it is supposed to be reference 37, but reference 37 is a different publication, a non-controlled report of nHFOV use, and I can’t find any link to a trial of nHFOV authored by Zhu in 2019, including from searching the Chinese database, CNKI. Also Liang 2019, and several other references, does not have a URL link; I searched the CNKI database and found a link to the Liang article, which had an abstract in English (the things I do for my readers!), but the full publication is behind a paywall, so I have no idea how extubation failure was defined in that study.
The systematic review seems to show that nHFOV post-extubation leads to a decrease in extubation failure from an overall rate in these studies of 1 in 4 with CPAP, (which seems very high) to about 1 in 9. In the studies comparing with nIPPV, the overall rate decreases from 1 in 6 with nIPPV to about 1 in 9 with nHFOV. But, if you eliminate the trials that I cannot find, and the tiny trial with an extremely high failure rate in controls, there is no clear advantage to post-extubation nHFOV compared with nIPPV in extubation failure.
The current evidence shows that prior to extubation babies we should ensure therapeutic caffeine treatment, perform a Spontaneous Breathing Test, and if the baby passes the test, very preterm infants should receive either nIPPV, nHFOV, or NIV-NAVA, with a PEEP of 6 if in 21% oxygen, and 8 or 9 if they have residual oxygen needs.
Decreasing extubation failure, and the need for reintubation, with its resultant trauma to the airways, and trauma to the parents hopes, is an important goal for research, even if longer term pulmonary complications are not affected.
About half of the babies already had an IV when they were enrolled. In the intervention group, babies then received “full-milk-feeds”, starting at 60-80 mL/kg/d (the published protocol states 60 mL/kg/d), whereas the control group had a maximum of 30 mL/kg/d enteral liquids on day 1.
This is described thus : “For infants in the full milk group, we started milk feeds within 3 h of birth at 60–80 mL/kg per day via a gastric tube and continued milk feeds without intravenous fluids or parenteral nutrition”. But this just isn’t true, 80% of the full milk group infants did have intravenous fluids on day 1, as their own figure shows. I think this is really just a question of wording, the full milk group babies were supposed to attempt full enteral nutrition, but large numbers of babies in this GA group will have expectant IV antibiotics for possible early onset sepsis, so they required IV access for good clinical care. 50% of the babies had an IV at enrolment (there is no mention anywhere in the publication or the supplementary materials of IV antibiotics). This also means that 300 babies in the full feeds group had an IV inserted, within the first few hours of birth, after they were assigned to the full enteral feeding group. This is never explained, or even mentioned or discussed.
They also never state what was done with feeding volumes for infants who had an IV running; were the IV fluids included in the fluid calculation? If a baby weighed 1.2 kg, for example, and had an IV running at 2 mL/h for their antibiotics, was the 40 mL/kg/d of IV liquid in addition to the enteral liquids? Or was that volume deducted from their feeds? This is an important detail given that 80% of the “full enteral” group had IV fluids.
After the initiation of the trial, the local care team could do whatever they wanted, in terms of increasing feed rate, or the source of additional feeds (donor milk or formula), or defining feed intolerance, or measuring gastric residuals(!), or timing of fortification. Full feeds were defined as at least 140 mL/kg/d for 3 consecutive days.
Forty percent of the “full enteral feeding” group had more than 24 hours of IV fluids, but again we have no idea how much of this was due to IV antibiotic use. The babies were all preterm, many had respiratory distress, more than a fifth had ruptured membranes for >24 hours, so I am sure that many had (and needed) IV antibiotics. On the other hand, there were 71% who were delivered by Cesarean section, and babies delivered by CS with intact membranes don’t need antibiotics.
I am sure some also needed IV dextrose for treating hypoglycaemia; we are told that the incidence of hypoglycaemia was the same between groups, but how many had an IV for low blood sugar on day 1 is not reported. In the supplemental data we learn that there were about 7% of babies in the full feeds group who “did not adhere to the protocol”, i.e. had intravenous fluids after 24 hours of age, who were in that situation because of hypoglycaemia. Also, 4% of the full feeds group had an IV after 24 hours of age for “other clinical reasons”, which I guess must include IV antibiotics, but that seems extremely low to me. 12% if them had an IV for not tolerating full feeds, and, as mentioned, 7% for hypoglycemia, In other words, nearly 90% of the babies did tolerate full feeds from birth.
The primary outcome was duration of hospitalisation, which was determined according to local practice. There was no impact of study group on the primary, just over 32 days in each group. There were also no differences in the secondary outcomes of NEC (which was rare, 4 cases vs 6 cases), or late-onset sepsis (which was uncommon, 3% vs 2%). Among gestational age subgroups, the primary and these secondary outcomes were similar.
There were differences in TPN use, number and duration of central line use, and the numbers of peripheral IVs inserted, as you would guess, these were all reduced in the early enteral feeds group.
My take away from this trial, and several other smaller trials, is that full nutritional support can be given, from birth, by the enteral route in a large proportion of preterm infants of 30 to 34 weeks, and if they have no other clinical indication for an IV access, one can completely avoid IVs. Infants who need IV antibiotics can usually have their antibiotics discontinued at 36 hours of age (because most of them have negative cultures), after which most of them can be on full enteral fluids. A number of recent trials, some of which I have discussed in the blog have shown the toxicity of TPN. These new data show that a large proportion of the 30 to 34 weeks babies (the majority of preterm babies in the NICU) can be managed without ever receiving TPN. They can also avoid the pain of IV insertion attempts, and the discomfort of IV infiltration episodes.
There does not seem to be any good reason to start at less than 60 mL/kg/d of enteral milk feeds in this group of babies on day 1. Some babies will have difficulty tolerating this, especially infants with IUGR, and in those babies you may need to slow down feeding advancement, or even sometimes to back down to smaller volumes or temporarily stop feeds. Some will also need IV glucose, but I can’t see any good reason for not at least trying to give full enteral nutrition from birth in these babies, even if they need IV access, and a small volume of crystalloid solution, for antibiotic administration.
I just learned of the very recent death of Dr Robert Hawkes Bartlett, May 8, 1939 – October 20, 2025. He was a surgeon who had been developing extracorporeal oxygenation systems for cardiothoracic surgery who realised that extracorporeal circulation could be used for prolonged support, and was willing to try it out for a baby who was dying.
“That child, treated in 1975 was.. a little girl. Her mother was just a girl herself. A Mexican peasant girl living in Baja who could neither read nor write and who realized, when she became pregnant in 1974, that her baby, if it lived at all, would fare no better. We all have hopes and dreams, and when we become parents our most fervent hope is that our children will live well, grow up bright and beautiful, and exceed the station of their parents, whatever that is. Poor Mexican mothers know that they can give the gift of opportunity to their new offspring in the form of United States citizenship by having the child born in this country. So it was that this young mother, consumed with the wish for a better life for her unborn child, crossed the border and set out for Los Angeles when her labor pains began. But as fate.. would have it, her water broke on the freeway and she took the next off-ramp to Orange County Medical Center. The baby was born – a perfect little girl- but something was wrong. The delivery had been difficult. The neonatologist tried to explain, “Mal respire. Mal grande. Intubation. Ventilator, Oxygen. Pressure. Hypoxia, Seizures.”
“The neonatologist knew that we were working with ECMO (rather unsuccessfully) with adult patients. Would we give it a try? The babe was dying. The arterial PO2 was 12. In the middle of the night, with the aid of a flashlight so as not to disturb the other patients, we tried to explain to the mother through an interpreter the ultimate in high tech procedures which had never been used successfully for an infant. She signed the consent form with an X, scared to death for her little girl and more scared that the official-looking form would bring recognition, deportation, perhaps imprisonment. She went in to see her baby girl, cyanotic, on a ventilator, with tense nurses and residents standing about. And the next day she disappeared, leaving her baby 2 gifts : a US citizenship and a name – Esperanza- Hope.
…we ligated the patent ductus arterosus and placed a catheter to monitor pressure in the pulmonary artery. This established the diagnosis of persistent pulmonary hypertension of the newborn. When the spasm finally relaxed and the blood flowed through the lung, our patient could be weaned off bypass, and off the ventilator. Soon she had a foster family.
The baby survived, and Ann Arbor started a program of offering ECMO for full term infants who were expected to die because of cardiorespiratory failure, usually hypoxic secondary to PPHN. They developed predictive criteria which were reasonably good at predicting which hypoxic babies under full intensive care would die, with over an 80% accuracy. But with ECMO they had over 80% survival.
Bob was criticized for not doing a randomized controlled trial, when introducing this new life-saving technology. Which could be likened to doing an RCT of parachute use when falling out of a plane (Yeh RW, et al. Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ. 2018;363:k5094); but nevertheless there were many sceptics in many parts of the world who thought they could have saved these babies without ECMO. He listened to them, and designed a study which minimized the number of potential deaths (Bartlett RH, et al. Extracorporeal circulation in neonatal respiratory failure: a prospective randomized study. Pediatrics. 1985;76(4):479–87). The “randomized play the winner” trial was a unique approach to a trial design, where potential adverse outcomes (death) were extremely likely. In essence, the first baby was randomized, and depending on whether they survived or died, the successive randomizations were weighted to increase the chance that a baby would be in the group with survivors, or decrease the chance of being in a group where the previous infant had died.
This design was likened to randomizing by pulling a ball from a sack, within the sack one starts with a black ball (ECMO) and a white ball (standard care). If a baby was randomized, to ECMO for example, and then survived, then an extra black ball was added to the sack prior to the next randomization. Likewise if the baby was randomized to ECMO and died, then an extra white ball would be added, or if they were randomized to standard care and survived. That way the previous “winner” group would have more chance of being the group assignment for the next baby. As it happened, the first baby was randomized to ECMO and survived (so a 2nd black ball was added) the second baby was randomized to routine care and died (so a 3rd black ball was added). This progressively increased the chances of a subsequent baby being in the ECMO group, and another 10 babies were randomized to ECMO who all survived. This reached the pre-specified success criterion, and the trial was terminated.
If this had been a standard RCT then 0/1 compared to 11/11 would not be “statistically significant”; by Fisher exact test the p value is 0.08. But it wasn’t designed as such a trial, and the results did exceed the pre-specified criterion for advantage of ECMO, without consigning large numbers of babies to the inferior treatment, or, to put it less politely, to die.
The observational data reported prior to this trial were already convincing enough for Neil Finer in our centre, and he went off for a few months to train in ECMO, then returned to Edmonton to start the first Canadian ECMO program, a process I was delighted to have a small part in.
A couple of years later we held an ECMO conference in Lake Louise, at which I got to meet Bob Bartlett, a delightful, thoughtful, humble man, you can detect those characteristics in the kindness of his description above of the dilemma of the mother of Esperanza.
The conference we held was in the winter, and the schedule was designed so that we could go skiing in the afternoons. Bob was a much better skier than I was, and I remember him skiing down the slopes, of the most beautiful scenery on earth, with his Sony walkman playing his favourite tunes as he skied.