
Pineda R, et al. Language and sound exposure across neonatal intensive care hospitalization and relationships with early outcome. J Perinatol 2026. In this short term outcome study, 64 very preterm infants <29 weeks GA were evaluated at near-term age with the Neonatal Neurobehavioural Score (NNNS). They had previously had a recording of the ambient noise for 4 separate 16 hour periods during their NICU stay, which was analysed to determine the exposure to any noise, including electronic sounds (which I guess means alarms, and monitors beeping), or meaningful language or distant voices.
The NNNS scores on the multiple various scales are shown below, with the “Comparator Value” being the average scores of full term infants, with the SD.
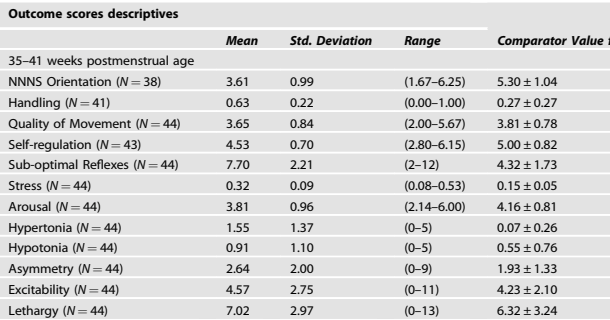
The statistically significant correlations with sound exposure and NNNS scores are shown below

Exposure to speech was associated with less stress, exposure to louder noise with more hypertonia, and so on.
In terms of statistics, this might be a bit questionable, as there were 5 sound characteristics and 13 different scales compared, leading to 65 possible associations, and a high risk of a type 1 error Nevertheless, the importance of human voices and the adverse impact of electronic sounds, especially loud sounds is consistent with everything else we know.
Take Home Message : Please get your parents, and everyone else, to talk calmly to the babies, and reduce as far as possible background noise and electronic sounds. Supplying books to parents, so that they can read to their infants while in kangaroo care, rather than scrolling on their phones, can only be a good thing.
In this multicentre observational study, infants with uncomplicated CoNS sepsis were compared between those with >96 hours of antibiotics. Cases were defined by “Presence of clinical signs of infection more than 72 hours after birth, a positive blood culture showing CoNS, and an increased C-reactive protein (CRP) level >10 mg/L within 24–36 hours after the onset of sepsis” and uncomplicated sepsis meant “clinical recovery within 24–48 hours, no central venous line in place or removed after the onset of sepsis, no signs of necrotizing enterocolitis or infected thrombus, and no Staphylococcus lugdunensis bacteremia”. (Apparently S. lugdunensis is particularly virulent). Most were treated initially with flucloxacillin and an aminoglycoside.
The primary outcome was the incidence of relapse of infection, and it was performed as a non-inferiority retrospective observational study.
There was one relapse in the short treatment group of 172 infants, and 0/218 in the long treatment group; short treatment satisfied the non-inferiority criterion.
Take Home Message : 4 days of adequate antibiotic treatment might well be enough for uncomplicated CoNS sepsis.
In the PREMOD2 trial, of delayed clamping vs cord milking for preterm infants at birth, some centres allowed waiver of consent and others did not. This study examines the differences in patient characteristics and the impact of the trial intervention between those 2 groups of centres.
When the study was designed and started, there was no evidence that one approach was preferable to the other, and some centres were doing DCC, others cord milking. If you remember, the trial found an increase in severe IVH with cord milking, leading to premature termination of the trial. There were 475 babies in total in the trial, 99 of them in hospitals that required pre-randomisation consent, the remainder in hospitals allowing waivers. “At hospitals permitting initial waiver, 3% of parents who were approached after the delivery intervention declined postnatal consent for data collection. At hospitals without initial waiver, 75% of deliveries were approached for participation. Among those approached, 49% of parents declined consent (range 39–61%)”.
In hospitals with a waiver, enrolled infants were more likely exposed to maternal chorioamnionitis (35% vs. 22%), less likely to have complete antenatal steroids (75% vs. 85%), and less likely to have received antenatal MgSO4 (79% vs 97%) compared to the others. Antenatal steroids and chorioamnionitis impacted the risk of having a severe IVH, mostly in the Cord Milking (UCM) group.
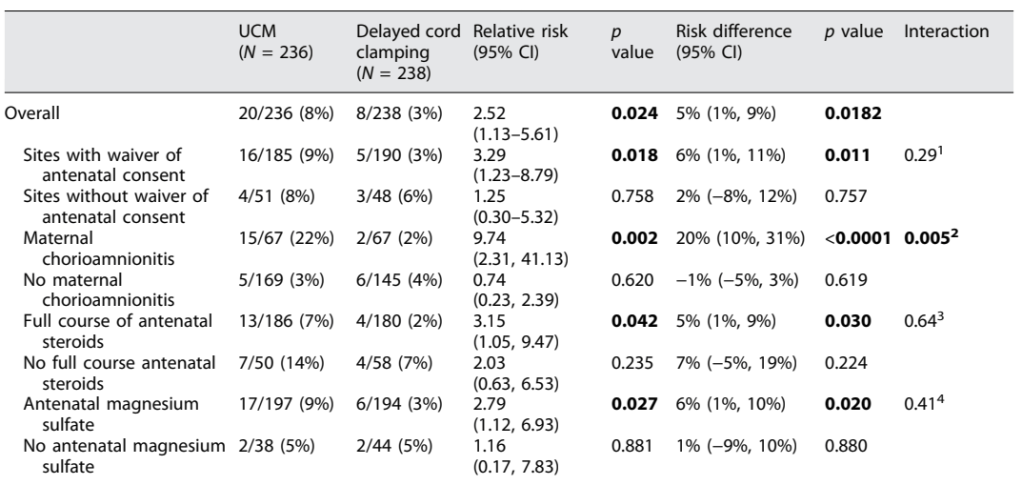
As you can see, in the cord milking group, antenatal steroids reduced the risk of severe IVH to 7%, compared to 14% without completed antenatal steroids, and Chorioamnionitis increased the risk from 3% to 22%.
Not having a waiver of consent therefore impacted the apparent difference between UCM and DCC, with waiver centres showing a decrease, and non-waiver centres showing no difference. This is probably because of the different risk profile among babies born in the different groups.
Our results highlight the importance of methods to enroll representative samples of the populations, to whom the studied interventions will ultimately be applied. Infants born to mothers that can be approached antenatally may have different comorbidities and co- treatments than the infants for whom the evidence will ultimately be applied… Relevant regulatory frameworks in countries including the USA and Australia have been previously described to support ethically appropriate modifications of the consent process for research on the safety and efficacy of common delivery room interventions. Based on the experience of PREMOD2, such methods may prevent false reassurances about safety or efficacy when unwarranted
There are previous data which confirm that parents questioned after the fact were supportive of this kind of waiver of consent. Even though 50% of those approached prospectively (in this trial) refused consent. I think that says something about how difficult it is in the midst of the stress of a threatened preterm delivery to explain comparative trials of differing approaches in common clinical use, which are both considered acceptable interventions.
Take Home Message : Waivers of consent, when ethically appropriate, allow randomization of subjects that more closely reflect the entire population. They may reveal effects of interventions which would otherwise be missed.






