
Since 2005 the International Committee of Medical Journal Editors has required that a condition of publication of a prospective controlled trial is that it should be registered in an accessible database prior to starting the trial. It is understandable that for a few years afterwards, trials that had been commenced prior to this standard might not have been pre-registered. I don’t think there is any reasonable excuse for not pre-registering prospective trials in more recent years.
Since 2013, the World Medical Association’s declaration of Helsinki has also clearly stated “Every research study involving human subjects must be registered in a publicly accessible database before recruitment of the first subject”.
Despite this obvious, basic, and easily complied with standard, many trials are still being performed without prior registration.
I recently wrote, for example, to the editors of “Neonatology” about this article Atef Abdelsattar Ibrahim H, et al. The Effect of Oral Immunotherapy on Preterm Neonates: A Promising Adjuvant Therapy in a Clinical Trial Study. Neonatology. 122.2025. p. 641–9. Which was a trial of oral colostrum. There were several major concerns that I had. The first was that the trial was registered after completion. This is inconsistent with the clear requirements of the ICJME and the WMA, and the stated criteria in the instructions of authors of “Neonatology”. The editorial board seem to be unaware of their own requirements.
In addition, the methods section of the trial does not describe the intervention. At all. It isn’t stated in the text that there were 3 groups, or that the groups had either no colostrum, 3 days of colostrum or 10 days of colostrum. The volume, frequency, and method of administration are not described.
In addition, the rate of early onset sepsis was enormous at 56% among the controls (and 10% in the 10 day group, 32% in the 3 day group) which is reported as if it was an outcome of the study. I think it is fairly obvious that a postnatal intervention cannot affect the incidence of early-onset sepsis, which should have been considered as a baseline imbalance.
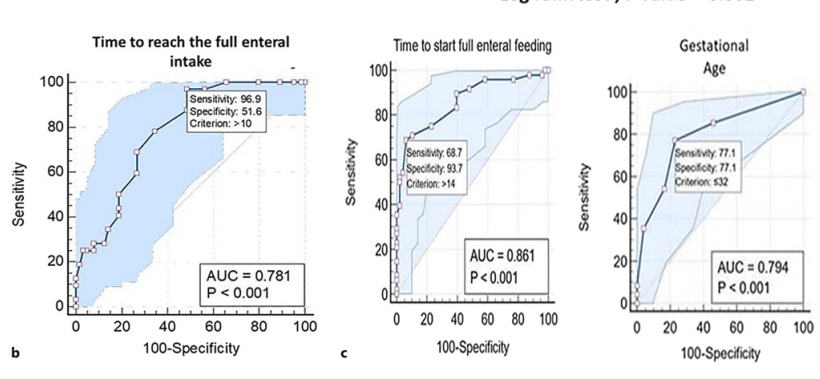
Some of the presentation of results is just plain weird. I’ll give a years free subscription to “neonatalresearch” for anyone who can explain to me what the following figure means! The figure legend states “b ROC curve of time to reach the full enteral nutrition for sepsis (sensitivity and specificity are expressed in %). c ROC curve of time to reach the full enteral nutrition for prolonged length of hospital stay (sensitivity and specificity are expressed in %), ROC curve for prolonged length of stay as regards GA (gestational age) (sensitivity and specificity are expressed in %).
The response of the editorial board of Neonatology was very disappointing. They stated that the authors had not been aware that they needed to pre-register their study. they also stated that the rate of sepsis was consistent with other studies in LMICs, and sent me a reference which included data about Late-Onset Sepsis. It seems that the referees and editorial board of Neonatology are also unaware of their own requirements.
One journal which has rejected multiple articles because of a lack of pre-registration is the BMJ. They recently published a study describing what happens to such articles (Blanco D, et al. Analysis of non-prospective trial registration in clinical trials submitted to The BMJ: observational study. BMJ. 392.2026. p. e086467). It turns out most authors just submit them elsewhere, “Many trials rejected by The BMJ for non-prospective registration in an ICMJE accepted registry were later published in high impact journals claiming adherence to the ICMJE recommendations, often without disclosure of registration deficiencies.”
The accompanying editorial in the BMJ, written by the same authors, offers suggestions:
Rather than simply describing the problems we encountered, we wanted to offer some practical steps to help improve transparency around trial registration. Journals can play a central role by requiring authors to provide clear, precise, and verifiable registration information in journal submission systems and in manuscripts. This should include the full dates (day/month/year) of submission to a trial registry, registry approval, and first participant enrolment, according to the latest registry entry. Journals should also require the trial registry name and registration number, a hyperlink to the registry entry, and a clear statement indicating whether the trial was prospectively registered in an ICMJE accepted registry. Trial registries must harmonise their language and terminology so that users can easily identify key milestones, such as the date of first submission, approval, and first patient enrolment, as well as clearly determine registration status.
On publication, prospective or retrospective registration in an ICMJE accepted registry should be clear from reading the abstract alone, with all registration information also reported in the full manuscript text. As Douglas Altman so wisely said in the 1990s, “Readers should not have to infer what was probably done, they should be told explicitly.” With the provision of these details, readers can make informed judgements about the credibility and transparency of the research for themselves.
Prior registration is an important safeguard that allows readers to be confident that the interventions, analysis, and outcomes were decided prior to seeing the results. Without pre-registration all of these things can be changed post hoc, which makes all of the medical research endeavour unreliable. Meta-analyses, on which many treatment decisions are made, based on such results may lead us to treat individual future babies with inappropriate, ineffective or dangerous therapies. Even individual small trials, which sometimes are the only evidence we have, must be pre-registered, and failure to do so, and failure of journals to insist that trials are pre-registered, puts our fragile patients at risk.






