
I wrote about this trial after last year’s PAS meeting, mentioning that it looked like a potential significant improvement in respiratory care of the preterm The full publication confirms that is a real possibility. McEvoy CT, et al. Extended Continuous Positive Airway Pressure in Preterm Infants Increases Lung Growth at 6 Months: A Randomized Controlled Trial. Am J Respir Crit Care Med. 2025;211(4):610-8.
The trial enrolled 100 preterm infants (24 to 32 weeks GA) who had at least 24 hours of CPAP and were considered ready to have the CPAP stopped (5 cmH2O, 21% O2, without tachypnoea or retractions or frequent apnoea, and tolerating breaks from CPAP during care procedures). They had to satisfy these criteria for 12 hours to be considered “stable”. (The pilot trial published previously used a pressure of 4-5 cmH2O, with the same criteria). They randomized the babies to their usual care, which was stopping the CPAP, or to remain on CPAP for a further 2 weeks. Neither this publication, nor the pilot, nor the registration documents, states what pressure was used for this extended CPAP treatment. Which I think is critical, did they use 4 or 8 cmH2O? or something in between?
Babies averaged about 30 weeks GA, and were eligible for the trial at a mean 32.4 weeks PMA, a minority in each group had required surfactant (25% vs 37%). Occasional infants paused the extended CPAP because of local nasal trauma, and occasional controls had to have their CPAP restarted.
Short term results confirmed the increase in FRC with prolonged CPAP, as demonstrated in the pilot, when measured just after the intervention period. At 6 months the infants had lung function testing, which showed improved Alveolar volume, improved DLCO, and better Forced Expiratory Flows.
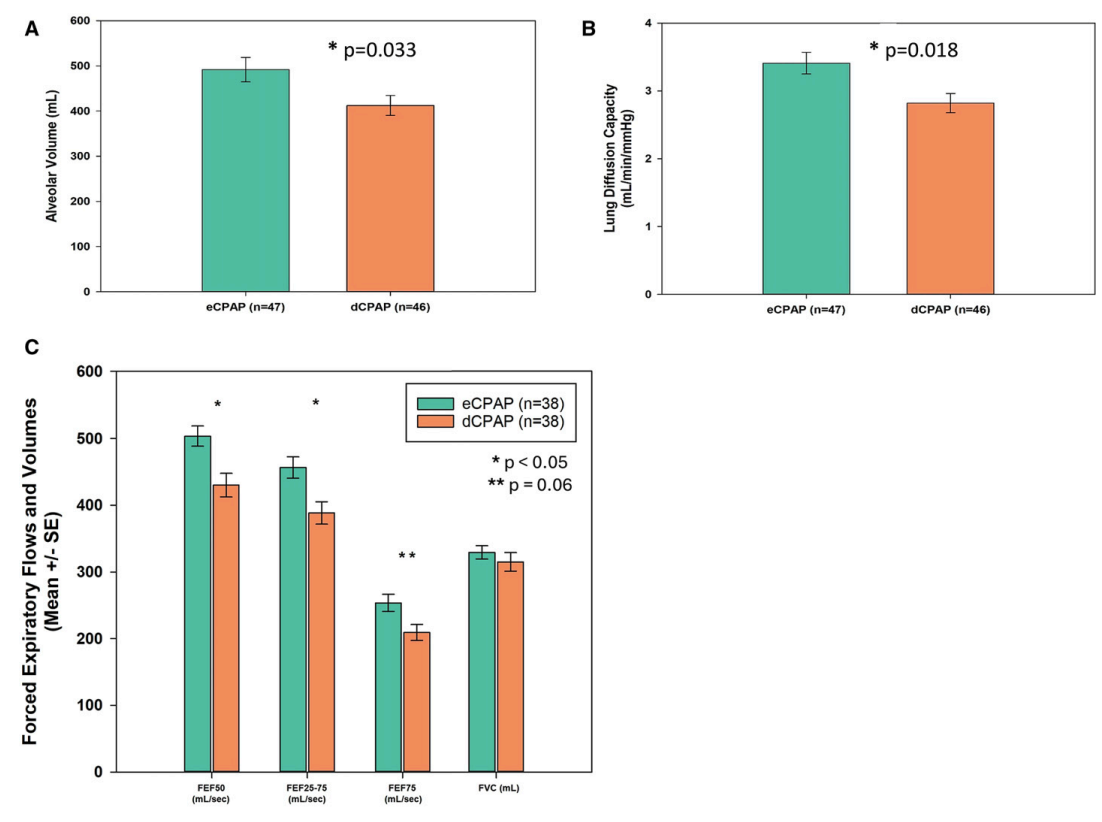
FEF is, of course, a measure of small airways function, and is frequently impacted by preterm delivery, this result is reassuring that the increase in alveolar volume is not just because the alveoli are distended, but probably lung growth overall is increased, including small airways. That would be consistent with findings from animal models; prolonged CPAP does not simply distend the lungs, it seems to promote lung growth, and, in a couple of models, decreases airway reactivity.
Parents were questioned about wheezing, and bronchodilator use. The questionnaire also asked about hospitalisations, and respiratory hospitalisations, but those data are not reported. Babies in the extended CPAP group were less likely to have wheeze, 43% vs 56%, but this is within the confidence intervals of no difference.
The major limitation of this trial, in terms of impact on clinical practice, is that these are babies with very little lung disease, only about 7% in each group had BPD, (Oxygen at 36 weeks). Although even such relatively minor lung disease of prematurity is known to lead to long term impacts on pulmonary health, whether the intervention would be equally as effective among infants with sicker lungs is unknown.
Routinely extending every baby’s CPAP by 2 weeks would have major impacts on resource utilisation, so we really need robust data. It also could have adverse impacts on oral feeding, especially breast feeding, during the time period when orality is also developing. Most of the babies in this study finished the intervention between 34 and 35 weeks, so the interference with developing breast feeding may have been small, but if babies who become eligible later (in terms of PMA) are treated with extended CPAP, the progression of breast feeding might be a major issue.
I hope that further trials, including infants requiring oxygen supplementation, and with more extensive analysis of outcomes of direct interest to parents, are planned. I also hope that the possible impact on breast feeding is investigated. If every very preterm baby, who is otherwise clinically ready to have their CPAP discontinued, will have that treatment extended for 2 weeks, we need to be very sure that the benefits justify the extra resources, and that there are no balancing negative effects.







CPAP improves FRC. And lung volume affects PVR through its influence on alveolar capillaries. So, the predominant mechanism for improved oxygenation overall and in the short term with CPAP is due to increased lung perfusion. But we know that lung architecture is not homogeneous. Ventilation is not uniformly distributed in the lung, in large part because of the effects of gravity. Because of the difference in alveolar volume at the apex and at the base of the lung, alveoli at the lung base are located along the steep portion of the pressure-volume curve, and they receive more of the ventilation (i.e., they have greater compliance). increased ventilation will cause low pCO2 in the capillaries and hence the alveoli. This reduction in pCO2 will be replaced by extra oxygen (as evidenced by alveolar gas equation) resulting in increased pAO2 (>100mmHg).This will result in increased PaO2 in alveolar capillaries in the dependent part of the lungs – Regional “Hyperoxia”.
Although the absolute amount of increased oxygen delivery may be insignificant if counted over a few breaths. But persistence of these mechanisms over days to weeks may potentially cause persistent vascular changes causing long term complications.
Please let me know your thoughts.
I have used nasal bubble CPAP in such infants for many years generally confined to 5-8 cm pressure with the higher being used for much shorter duration than the lower values. Of course, some of these infants have also been dosed with surfactant at the beginning or early in their CPAP course. I’ve found that the infant’s tolerance and response has generally been excellent. However, the one complication which I’ve encountered that doesn’t seem to be mentioned and can not only interrupt the plans for treatment course and duration as well as add significant morbidity is an air leak. Did I miss that ? This is particularly prevalent after surfactant dosing (change in compliance and easier over distention of alveoli) and in the improvement phase of CPAP therapy in general. It seems to be more of problem in the older, more active preterms who don’t always agree that something blowing a lot of gas into their nose is such a great idea and the agitation/crying creates more significant pressure differentials.
It would be important to compare baseline saturation and pCO2 values when doing a larger study. Also bubble CPAP vs nasal cannula CPAP, and various brands etc., are not exactly equivalent. Different centers have different devices that may not deliver the same outcomes or have the same risks. Infants would remain at a critical care coding level for longer, but significant long-term benefits could justify this.
Stretching other parts of the body, such as two ends in esophageal atresia (Foker), or fetal tracheal ligation in congenital diaphragmatic hernia, etc., can induce growth. Ventilation/perfusion also need to be taken into account.