
In my previous post about hypoglycaemia, I made certain estimates about the proportion of well-appearing term and late preterm babies who would be considered at-risk. Karen Puopolo and her group at the Pennsylvania hospital have just published a study covering over 10,000 infants delivered at 36 weeks or later. This retrospective study reports the proportion of babies considered at-risk, which included SGA, >4kg, preterm, post-term (over 41 weeks) infants of diabetic mothers or those who had beta-stimulants or beta-blockers. (Mukhopadhyay S, et al. Clinical impact of neonatal hypoglycemia screening in the well-baby care. J Perinatol. 2020.)
The first finding of importance is that nearly 50% of all deliveries (48.7% to be exact) were considered to be at risk and were therefore screened. The study includes babies who were screened because of non-specific signs that were perhaps due to hypoglycemia, that is, a baby who is a bit jittery or is found with a lowish temperature is often (and should be) screened for hypoglycemia; these infants were about 2000 of the 5,140 screened infants in the study. These figures highlight the importance of the definition of who is at risk; subtracting the babies who were only screened for possible symptoms, over 30% of late preterm and full-term babies qualify for screening.
The clinical definition of hypoglycemia used for most of these infants was 2.78 mmol/L (50 mg/dl) at all time points, but after the first 18 months of the study the threshold for the first glucose at 2 hours of age or less, according to their protocol, was reduced to 2.5 mmol/L (45 mg/dl) for the remaining 14 months of this study period.
Using these definitions 43% of all the screened infant had at least one hypoglycaemic blood glucose (by bedside stick testing- Accu-check), and received an intervention (usually an extra feed of some sort) before 72 hours of age (when data analysis for this study finished).
Overall, 52% of the infants of diabetic mothers had at least one glucose <2.78, and 42% of the others. Of the babies screened for possible symptoms, 31% had a blood sugar between 2.0 and 2.78 mmol/L at some point, although very few needed extensive treatment and NICU admission.
In other words, using these definitions nearly one quarter of healthy newborn babies, born at term or late preterm, were considered abnormal. One of the adverse consequences of this is that extra feeds are often not breast milk, so among the 3/4 of mothers who planned to breastfeed, 3/4 of them received formula if they had a blood glucose under 2.78 mmol/L. Of those who never had a blood glucose below 2.78 then 56% were exclusively breastfed.
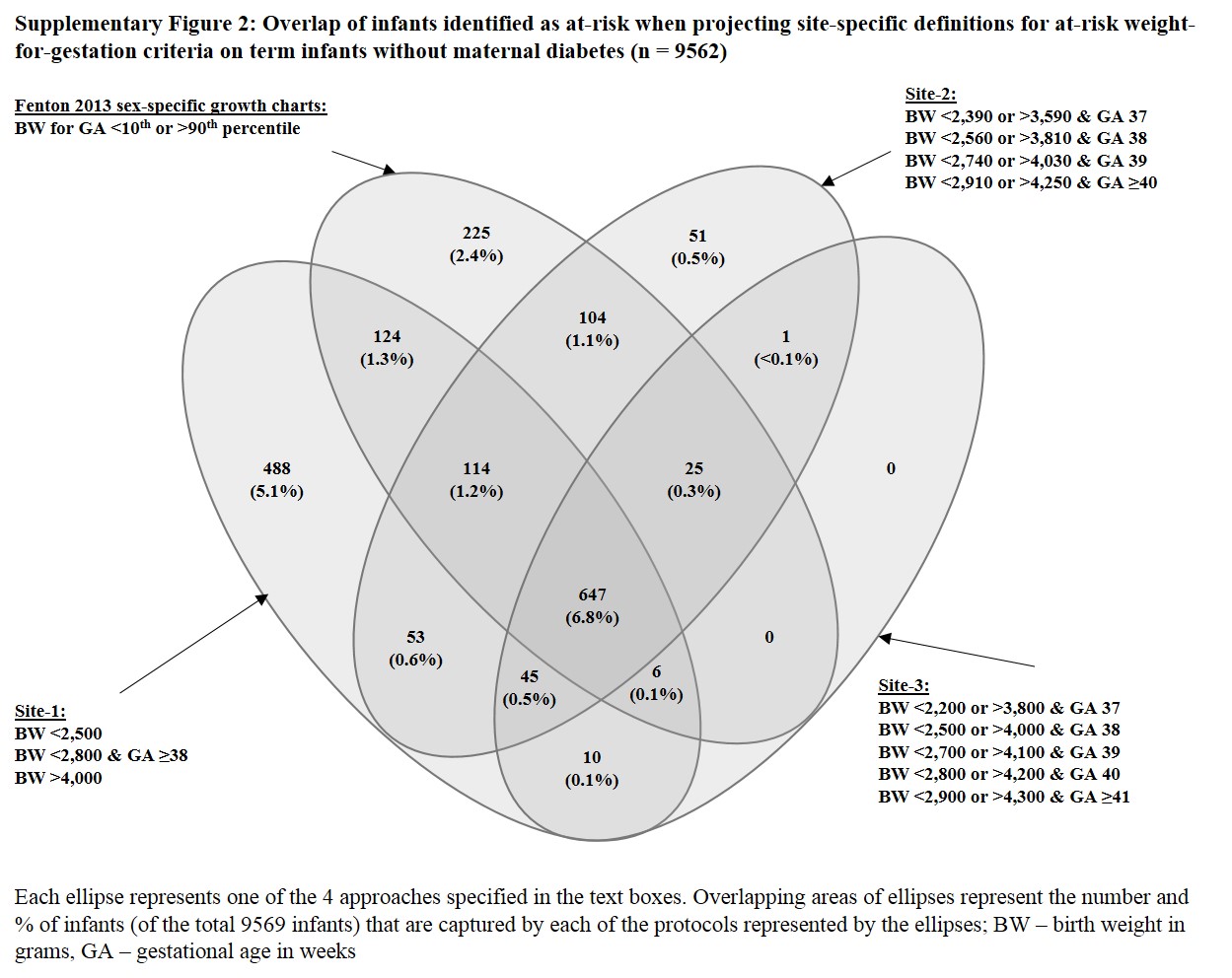
The authors also examine which criteria identify which infants for screening, and compare criteria from 3 different hospitals as well as using the Fenton charts.
The figure below shows how they overlap; it is interesting that the Fenton charts identify a total of only 13.2% of babies as being either under the 10th or over the 90th percentile. I guess that there is a high proportion of LGA babies who are infants of diabetic mothers and thus not included in this group.
A big limitation of this study is the reliance on the Accu-chek device for blood glucose monitoring, which means that there is likely an overdiagnosis of hypoglycemia, as bedside devices all have inaccuracies and tend to read lower than the true concentration.
I think it is still somewhat unclear whether LGA babies whose mothers are not diabetic really require screening. Some studies suggest that they do indeed, but the adequacy of antenatal screening and the criteria used for the diagnosis are not clarified in several studies I found, it does seem that mothers with impaired glucose tolerance, even if not satisfying standard criteria, have babies who are larger than average, and who may be at risk. More work is needed, I think.
Using more restricted, and physiologically relevant thresholds for making a diagnosis of hypoglycemia has several potential benefits, born out in the hypoEXIT trial: fewer babies with a diagnosis, fewer babies receiving unnecessary supplemental feeds, which are usually not maternal breast milk, less separation of mothers and babies.
It is important that we also find ways to reduce the proportion of babies who are screened, as well as having a more evidence-based threshold for treatment.Those babies are also adversely affected by the blood draws, repeated testing to confirm low point of care tests, overtreatment while awaiting confirmation, and all of the impacts which happen to screened babies, even those who are never hypoglycemic.
We need to go beyond the rather 20th-century method of putting babies on a scale at birth to determine their risk of having too little glycogen or too much insulin.
Perhaps intra-uterine growth restriction could be flagged by the obstetricians using deviations from their intrauterine growth curves on sequential ultrasound, many mothers already have a scan at 20 and at 36 weeks, and we could probably eliminate many small babies who are not growth restricted.
At the other end of the weight scale, babies of mothers with completely normal GTT and a large baby could probably avoid being poked by nurses or lab techs.







Pingback: Glucose screening and treatment in the newborn; what now? | Neonatal Research