
Seems like a dumb question I know, if they work in one country, surely they should work everywhere? It is sometimes difficult, however, to institute change based on studies that are done elsewhere, usually because there is an idea, or some evidence, that risk factors and other co-interventions may be different in published trials from local practice. Based on the results of the high-quality PIPS trial (multicenter RCT in the UK testing B. breve against placebo for prevention of NEC which did not show an impact), many centres in the UK have been reluctant to introduce probiotic supplementation.
A newly published cohort study from Norwich shows that there are some UK centres that have nevertheless introduced routine probiotic supplementation (Robertson C, et al. Incidence of necrotising enterocolitis before and after introducing routine prophylactic Lactobacillus and Bifidobacterium probiotics. Arch Dis Child Fetal Neonatal Ed. 2019:fetalneonatal-2019-317346). In 2013 they introduced probiotic prophylaxis, and they have seen an immediate and persistent reduction in NEC, using, at first, a preparation with 2 organisms, and more recently a preparation with 3 organisms, including a B longum sbsp infantis. They found more than a 50% fall in NEC after introducing probiotics, a decrease which was sustained, and did not seem to be associated with any other changes in practice. Breastfeeding frequency was stable, and they performed multiple analysis to try and confirm whether or not the probiotics were likely to be the main change associated with NEC reduction, no other obvious explanation was found. They evaluated the effects in multiple subgroups.
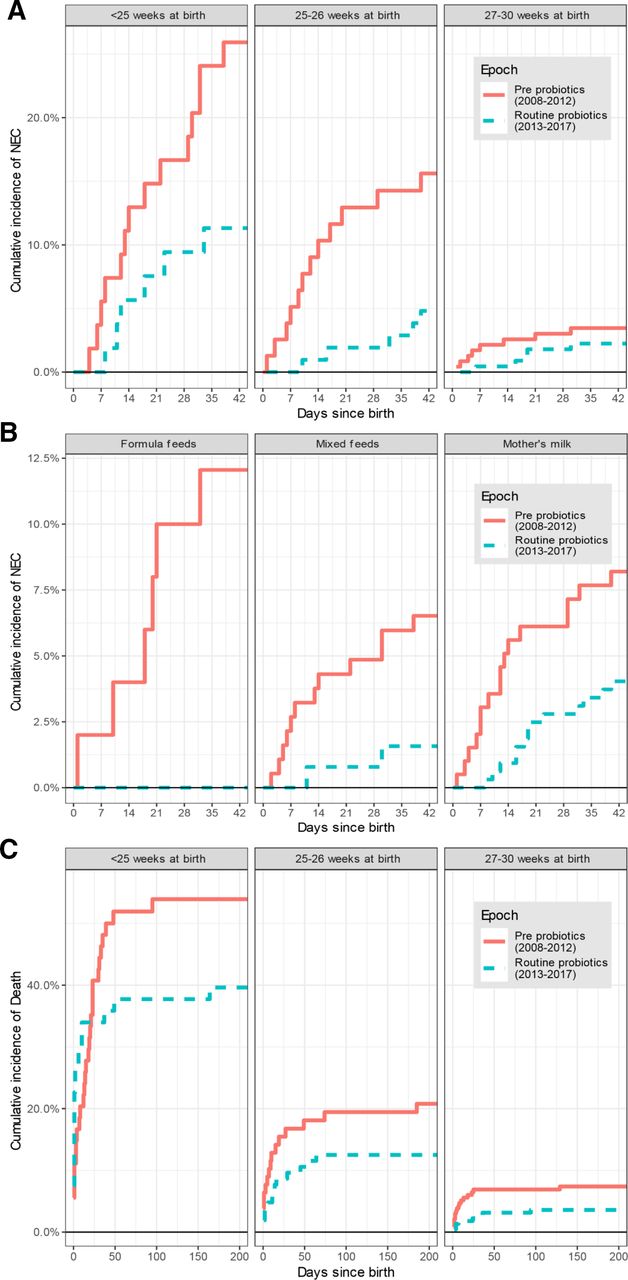
For the impact of diet, there were no cases of NEC among babies who received exclusively donor milk, but before you get excited about that, there were only 9 of them; there also weren’t many who got only formula (the group with the most dramatic impact in the figures above); 50 infants pre-probiotics, and 23 post. The majority had either exclusive breast milk or a mix of breast-milk and other sources.
There is some reason to believe that B. infantis is one of the most important of the probiotic organisms, and systematic reviews now generally show that a combination of probiotic organisms is more effective than a single strain. (Hagen PC, Skelley JW. Efficacy of Bifidobacterium Species in Prevention of Necrotizing Enterocolitis in Very-Low Birth Weight Infants. A Systematic Review. J Pediatr Pharmacol Ther. 2019;24(1):10-5).
Many of those combinations contain a Bifidobacterium which is at least similar to B infantis.
Promoting and supporting colonization with B. infantis and doing what we can to normalise the intestinal microbiome of the very preterm infant is a goal which seems to bear fruit. Finding better ways of doing this and reducing colonization with pathogens are important goals for the future. Testing the appropriate prebiotic molecules to support the growth of B. infantis, such as 2′-fucosyl-lactose should be a priority.






