
Systematic reviews, and meta-analyses should help us make a clinical decision, by accumulating all the evidence, determining its quality, and synthesizing impacts, we can then decide which therapeutic option to pursue. This latest review answers the following question “should I give intrapulmonary steroids to this preterm baby, who is somewhere between 0 and 14 days of age, and has either just been intubated for surfactant or is maybe still intubated because of early chronic pulmonary dysfunction”, In other words a question no-one has ever asked. (Delara M, et al. Efficacy and safety of pulmonary application of corticosteroids in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Archives of disease in childhood Fetal and neonatal edition. 2019;104(2):F137-F44).
This SR therefore fails Barrington’s test, which is based on Barrington’s rule, “if an individual baby could not be eligible for the 2 or more trials which are included in an SR, don’t meta-analyze them”. The results are meaningless. Worse they are misleading, as this SR implies that pulmonary administration of steroids safely reduces BPD frequency, no matter how or when they are given.
(This isn’t the first time, I have written about this issue : https://neonatalresearch.org/2016/02/24/steroids-directly-in-the-lungs-version-2/)
This is also another publication with poor editing and galley proof revision. The rather humorous result being that 2 studies apparently administered influenza to their babies!
(I presume some junior copy editor was very pleased with themselves when they replaced FLU by influenza, without realizing that it was actually an abbreviation for fluticasone!)
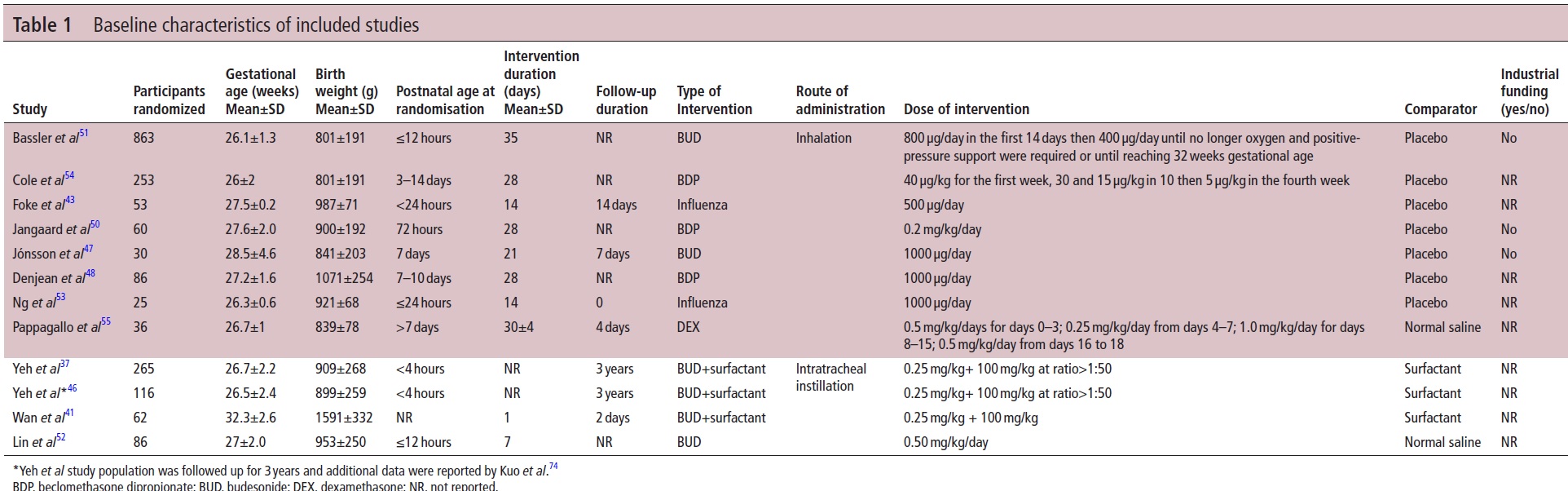
They have also completely misrepresented the dose of inhaled dexamethasone in the trial by Pappagallo et al, they don’t seem to have realized that the two phases of the trial were performed on different patients. But, as there are no results presented from that trial anywhere in the review (reported outcomes are pulmonary function tests), I guess it is not that important.
What would be worthwhile is a systematic review that divided these interventions into groups with fairly similar eligbility criteria, such as babies recently intubated for HMD support, babies who do not drop to 21% oxygen after their surfactant treatment, or babies still ventilated at a 7 to 10 days of age.
Meta-analysis of multiple small studies is already problematic; multiple small studies, 3 medium sized studies and 1 large multicenter trial, which include completely different groups of babies, should not be analyzed together.
Let us also not forget that the NEUROSIS trial, referred to as Bassler et al in this systematic review, showed an increase in mortality. 82/413 inhaled budesonide babies died, compared to 58/400 placebo infants. Bassler D, et al. Long-Term Effects of Inhaled Budesonide for Bronchopulmonary Dysplasia. The New England journal of medicine. 2018;378(2):148-57.
Delara et al wrongly state that the longest follow up for mortality was 35 days, whereas Bassler et al report death to discharge and then to 18 to 22 months when follow up examinations were performed.
Just as important is that this review, as many others, supposes that having fewer babies on oxygen at 36 weeks is an important goal in itself. BPD, by this definition, has very little correlation with long term pulmonary health. Indeed, steroids impair lung growth and development, so having lower oxygen requirements at 36 weeks may not translate to better pulmonary outcomes. Decreased early inflammation could be associated with impaired lung growth and alveolarization, so clinically important pulmonary outcomes must be studied before we universally start routinely putting steroids into the lungs of preterm babies.






