
In response to my previous post, one of the comments was a question about fluid volumes in the first few days of life, and whether fluid and/or sodium intake was important for the development of BPD during the early neonatal transition.
In response I will share a slightly edited preprint version of a section of an article I published in Seminars in Perinatology a couple of years ago. Barrington KJ. Management during the first 72h of age of the periviable infant: An evidence-based review. Seminars in Perinatology. 2014;38(1):17-24.
Even though it is a couple of years old, I don’t think there are new RCTs addressing the issues that I reviewed in this section. That article also had sections on cardiovascular support, respiratory management, nutrition, neurologic interventions, protocolized care and research networks.
Also it is important to note that the “systematic reviews” were performed according to the usual standards, but they do NOT conform to the PRISMA guidelines. With the limited space available I couldn’t have done that.
Fluids, electrolytes and renal function
Renal vascular resistance is high immediately after birth, and falls rapidly in the first 24 hours. This fall is associated with a major increase in glomerular filtration rate, and urine output, which is usually clinically evident as an increasing diuresis by the end of the 1st 24 hours of life. After this transition, preterm renal function is marked by a low ability to excrete a sodium load, but little restriction in maximal water clearance.
There are few studies on which to base a decision regarding total fluid management in the extremely immature newborn (EIN). The skin of the very immature infant is very permeable, and huge trans-epidermal water losses (TEWL) occur if they are placed in a dry environment, the evaporation of water from the skin of the infant leads to cooling due to the latent heat of vaporisation, and it may be impossible to keep the EIN warm in a dry environment under a radiant heater. Most centers have now moved to placing EINs in incubators, although there is no RCT evidence that this is preferable to being under a radiant heater, it seems likely to be the case. If a radiant heater is used it must be combined with an arrangement to keep the humidity around the infant at a high concentration, such as covering the infant with plastic.
One problem with keeping EINs in a high humidity environment is that whenever they are accessed to give care (for example by opening the incubator portholes) the humidity drops precipitously. This is even more evident when the ‘roof’ of an incubator with a retractable cover is lifted. Therefore further methods to reduce trans-epidermal water loss have been examined, including using ointments or semi-permeable membranes. Ointments such as Aquaphor can reduce trans-epidermal water loss, but whether they can improve overall water balance or improve clinical outcomes is uncertain. The only large study in ELBW infants enrolled infants (500 to 1000 g birth weight) starting at an average of about 24 hours of age, and showed an increase in late-onset coagulase negative staphylococcal sepsis during prolonged treatment . Maturation of the epithelial barrier after preterm birth occurs rapidly, a briefer period of barrier treatment could potentially have benefits without this risk. Semi-permeable membranes have also been tried, in a small pre-post study TEWL appears to have been reduced, fluid requirements and peak sodium was lower, and there may have been less BPD, (n=69 birth weight <1000g) but there is no data from adequately powered RCTs examining other clinical outcomes.
Total fluid intake
What should the total fluid intake be? Clearly this will depend on overall fluid losses. But the interaction between the physical environment, and subsequent TEWL, and fluid administration requirements has not been well studied. Several studies have randomly compared infants by total volume of fluid administered. The results are very inconsistent. Those studies have varied in design, in particular by how sodium intake was controlled.
Although the Cochrane review “Restricted versus liberal water intake for preventing morbidity and mortality in preterm infants” suggests that restricted fluid intake improves several clinical outcomes, this result is marked by significant heterogeneity, also one of the better studies did not enrol babies until the 3rd day of life, and therefore is of little relevance to the current review. After the initial period of adaptation as mentioned above, the preterm kidney has a relatively good ability to clear a fluid load. Thus there is little reason to hypothesize that variation in total free water administration, within reasonable limits, will affect total body water.
One of the 5 trials of water restriction gave fluids with identical sodium concentrations in each 100mL of the intravenous fluid, another was designed to examine a relatively complex protocol allowing either 10% or 15% body weight loss and therefore varied both water and sodium intakes. These 2 studies were therefore studies of combined sodium and water restriction.
I have performed a systematic review of RCTs of different fluid administration rates starting on the first day of life, which I have meta-analyzed using the RevMan software, fixed effects model. I found 5 controlled trials (a table showing the articles is at the bottom of this post, followed by a list of references), 3 of which had similar sodium intakes in each group, 2 varied both the fluid and the sodium intake.
Figure 1.Effects of varying fluid intakes on mortality.

As can be seen, the studies with varying water intake, but no difference in sodium intake showed no effect on mortality, whereas those which varied both showed a reduction in mortality with restricted water and sodium intake. Of note this second result is largely the result of a single trial with a very high mortality in the high water/high sodium group, and this subgroup shows substantial heterogeneity, an I2 of 72%.
Figure 2. Effects of varying fluid intakes on BPD
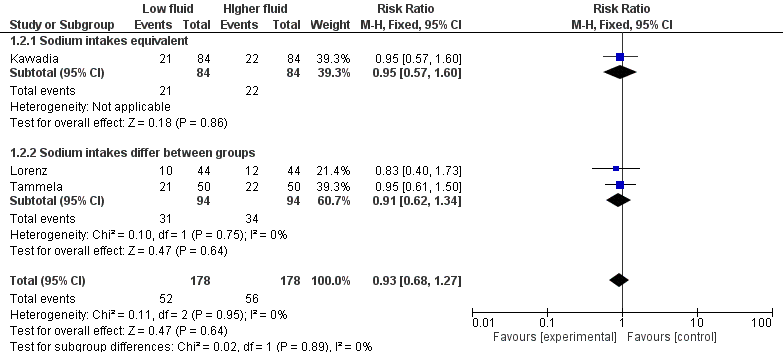
Clearly there is no effect on BPD, RR 0.93 (95% CI 0.68, 1.27). Survival without BPD was also not different overall.
Sodium intake
In contrast the preterm kidney has a limited ability to excrete a sodium load, and excessive sodium administration may lead to increases in total body water and increases in water content of vital tissues. This is true even though there is a natriuresis in the first few days of life, at least after the first 24 hours, which accompanies the postnatal diuresis. Administration of sodium during this period may well upset the postnatal progressive decrease in extra-cellular fluid which is a normal phenomenon in more mature infants.
I performed a systematic review and meta-analysis of RCTs in preterm infants which compared 2 regimes of sodium administration starting on the first day of life (see the table below). The search found 5 studies, two of which are as mentioned also studies of varying water intake and are mentioned above, and one with very limited description of clinical outcomes (other than death). The total numbers of infants in these trials is a disappointing 271. Nevertheless there appears to be a reduction in mortality RR 0.44 [95% CI 0.22, 0.90] with reduced sodium intake, a possible reduction in BPD, RR 0.76 [95% CI 0.56, 1.04] and a reduction in the combined outcome of death or BPD, RR 0.39 [95% CI 0.23, 0.67].
Figure 3. Effects of different sodium intakes on A. mortality, B. Bronchopulmonary Dysplasia, and C. combined outcome of death or BPD.
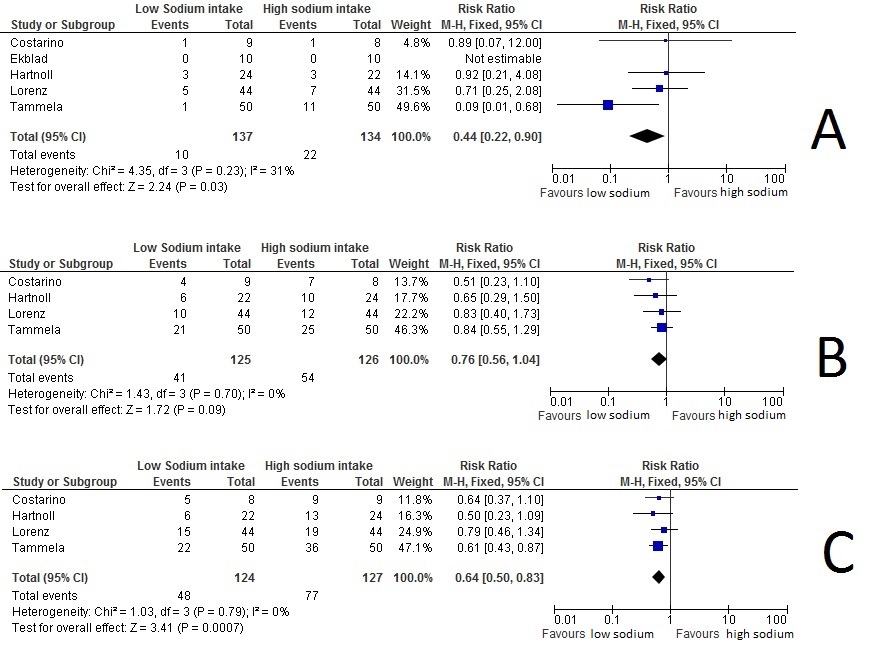
The data are therefore probably best interpreted as showing that delaying all sodium intake until after either 3 days of life or after a 5% weight loss improves outcomes whereas restricting free water intake by itself has little or no effect. The major limitation of these data being that very few extremely immature babies have been included in any of these studies.
Table Randomized trials comparing 2 levels of fluid intake or 2 levels of sodium administration in the preterm.
Study ID |
n |
Characteristics of included infants |
Comparison, fluid intakes |
Sodium intakes |
Primary Outcome |
Tammela9 |
100 |
<1751 g BW, >23 wk |
50,60,70,80,90,100,120 then 150 ml/kg/d vs80,100,120,150 then 200 ml/kg/d |
3 mM/100 mL Na in all the fluids |
BPD |
Lorenz12 |
88 |
750-1500 g BW, day 1 of life |
Designed for 10% birth weight loss vs 15%, initially1,000-1,500g 70 ml/kg/d 750-1,000g 80 ml/kg/d. Thereafter varied according to weight loss. |
Higher in high fluid group, 1 mM/kg/d on day 1 increasing to 3 in high fluid group or decreasing to 0.5 in low fluid group, by day 4 |
No clear primary outcome |
Von Stockhausen13 |
56 |
Premature, day 1 of life |
60 mL/kg/d vs 150 mL/kg/d for 3 days |
unclear |
No clear primary outcome |
Kavvadia14 |
168 |
<1501 g BW, day 1 of life |
70 increasing to 150 by day 6, 40 increasing to 150 by day 7 |
Adjusted to achieve serum concentration of 135 to 145 mM/100mL, no difference between groups |
Survival without BPD |
Costarino15 |
17 |
<1000g, <29wk, day 1 of life |
Individualized, not different overall between groups |
0 vs 3 to 4 mM/kg/d |
Risk of hypernatremia and large fluid volumes |
Hartnoll16 |
46 |
25 to 30 wk with RDS |
Individualized, not different between groups |
4 mM/kg/d starting on day 2 vs 0 until weight decreased by 6% |
Risk of continuing oxygen dependency |
Ekblad11 |
20 |
<35 wk |
50 increasing to 110 in each group |
0 increasing to 2, vs 4 mM/kg/d |
No clear primary outcome |
References
- Lorenz JM, Kleinman LI, Ahmed G, Markarian K. Phases of fluid and electrolyte homeostasis in the extremely low birth weight infant. Pediatrics. 1995;96(3 Pt 1):484-9.
- Pabst RC, Starr KP, Qaiyumi S, Schwalbe RS, Gewolb IH. The effect of application of aquaphor on skin condition, fluid requirements, and bacterial colonization in very low birth weight infants. J Perinatol. 1999;19(4):278-83.
- Knauth A, Gordin M, McNelis W, Baumgart S. Semipermeable polyurethane membrane as an artificial skin for the premature neonate. Pediatrics. 1989;83(6):945-50.
- Nopper AJ, Horii KA, Sookdeo-Drost S, Wang TH, Mancini AJ, Lane AT. Topical ointment therapy benefits premature infants. The Journal of pediatrics. 1996;128(5 Pt 1):660-9.
- Edwards WH, Conner JM, Soll RF, for the Vermont Oxford Network Neonatal Skin Care Study Group. The Effect of Prophylactic Ointment Therapy on Nosocomial Sepsis Rates and Skin Integrity in Infants With Birth Weights of 501 to 1000 g. Pediatrics. 2004;113(5):1195-203.
- Bhandari V, Brodsky N, Porat R. Improved Outcome of Extremely Low Birth Weight Infants with Tegaderm[reg] Application to Skin. 2005;25(4):276-81.
- Bell EF, Acarregui MJ. Restricted versus liberal water intake for preventing morbidity and mortality in preterm infants. Cochrane database of systematic reviews (Online). 2008(1):CD000503.
- Bell EF, Warburton D, Stonestreet BS, Oh W. Effect of fluid administration on the development of symptomatic patent ductus arteriosus and congestive heart failure in premature infants. The New England journal of medicine. 1980;302(11):598-604.
- Tammela OKT, Koivisto ME. Fluid restriction for preventing bronchopulmonary dysplasia? Reduced fluid intake during the first weeks of life improves the outcome of low-birth-weight infants. Acta Paediatr. 1992;81:207-12.
- Drukker AMDP, Guignard J-PMD. Renal aspects of the term and preterm infant: a selective update. Current Opinion in Pediatrics. 2002;14(2):175-82.
- Ekblad H, Kero P, Takala J, Korvenranta H, VÄLimÄKi I. Water, Sodium and Acid-Base Balance in Premature Infants: Therapeutical Aspects. Acta Pædiatrica. 1987;76(1):47-53.
- Lorenz JM, Kleinman LI, Kotagal UR, Reller MD. Water balance in very low-birth-weight infants: relationship to water and sodium intake and effect on outcome. The Journal of pediatrics. 1982;101(3):423-32.
- Stockhausen H, Struve M. Die Auswirkungen einer stark unterschiedlichen parenteralen Flüssigkeitszufuhr bei Früh- und Neugeborenen in den ersten drei Lebenstagen. Klinische Pädiatrie. 2008;192(06):539-46.
- Kavvadia V, Greenough A, Dimitriou G, Hooper R. Randomised trial of fluid restriction in ventilated very low birthweight infants. Archives of disease in childhood Fetal and neonatal edition. 2000;83:F91-F6.
- Costarino ATJ, Gruskay JA, Corcoran L, Polin RA, Baumgart S. Sodium restriction versus daily maintenance replacement in very low birth weight premature neonates: a randomized, blind therapeutic trial The Journal of pediatrics. 1992;120(1):99-106.
- Hartnoll G, Betremieux P, Modi N. Randomised controlled trial of postnatal sodium supplementation on oxygen dependency and body weight in 25-30 week gestational age infants. Arch Dis Child Fetal Neonatal Ed. 2000;82(1):F19.






