
Although many people (including myself) are convinced that human breast milk is the preferable nutrition for human babies, including the preterm, some of the evidence regarding benefits is shaky. For example the evidence that breast milk feeding reduces late-onset sepsis. The Cochrane systematic review by Bill McGuire and first author Maria Quigley Quigley M, McGuire W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane database of systematic reviews (Online). 2014;4:CD002971. for example found 2 trials that reported the outcome, with no significant difference between donor breast milk and formula, RR 1.12 (95% CI 0.84 to 1.49). Of course, as my gentle readers will be well aware, absence of evidence is not the same as evidence of absence. Which means that breast milk might really reduce infections, we just haven’t proven it (or it might not).
There is so little “equipoise” that it is difficult to get good trials done, partly because the evidence regarding NEC pushes us to promote donor milk if you have it available. Again from a strict scientific viewpoint the evidence is not that strong, a few small trials, none of which are significant individually, according to the above Cochrane review, but together there is a possibility of a benefit, RR of NEC with formula 2.77.

The effect of an intervention when there are multiple small trials is often exaggerated, a trial sequential analysis might well show no significant difference, but I don’t have the energy to do that right now.
Other comparisons show other benefits of breast milk (mostly with mother’s own breast milk), but there also concerns about short term growth, with either maternal or donor breast milk.
Having said all that, I have to note that I am very happy that Quebec now has a government funded human milk bank, that gives us very high quality product, and I am ready to give it to all the babies at risk of NEC whose mothers can’t produce enough milk. If breast milk were an expensive drug, with possible side effects, to prevent NEC I’d say the data are not sufficient. But breast milk doesn’t have much of a down side, apart from potential growth effects and maybe CMV, and processing it according to the latest standards gets to be expensive. It also just makes a lot of sense.
I should, of course, note that Hema-Quebec do process the milk, but the “product” is the fruit of the dedication of milk donors around the province who selflessly, and freely, and anonymously, donate their milk to help our preterm babies. Thank you so much donors!
So why the title of this post? Partly because of this study:
Corpeleijn WE, et al. Effect of Donor Milk on Severe Infections and Mortality in Very Low-Birth-Weight Infants: The Early Nutrition Study Randomized Clinical Trial. JAMA Pediatr. 2016. Nearly 400 VLBW infants were randomized to receive either formula or banked donor breast milk if the mother didn’t provide enough milk. Only infants who had never had formula were eligible, and most babies were in the trial and randomized and receiving their first feed by 6 hours of age. The primary outcome of the study was the composite incidence of NEC, serious infection (blood culture positive sepsis or meningitis), or all-cause mortality between 72 hours and 60 days of life. The main problem with the study is that the intervention only lasted 10 days, after which babies who needed supplements to mother’s milk all received formula. The breast milk was not fortified during the first 10 days either group.
The authors explain why the study intervention period was only 10 days, the need to fortify breast milk to supply adequate nutrition, and that the only fortifiers available to them are cow’s milk based. They wanted to examine the effects of a period with no cow’s milk exposure.
The primary endpoint was not different between groups, not even a little bit.
As the authors note, about half of the primary outcome determinations were before 10 days of age, but this design does still have major limitations.
Kreissl A, et al. Human Milk Analyser shows that the lactation period affects protein levels in preterm breastmilk. Acta Paediatr. 2016;105(6):635-40. Preterm breast milk protein content soon after initiating lactation is higher than later on. This is new data confirming that, and graphically showing how enormously variable the protein concentrations are. One was only 0.2 g/L
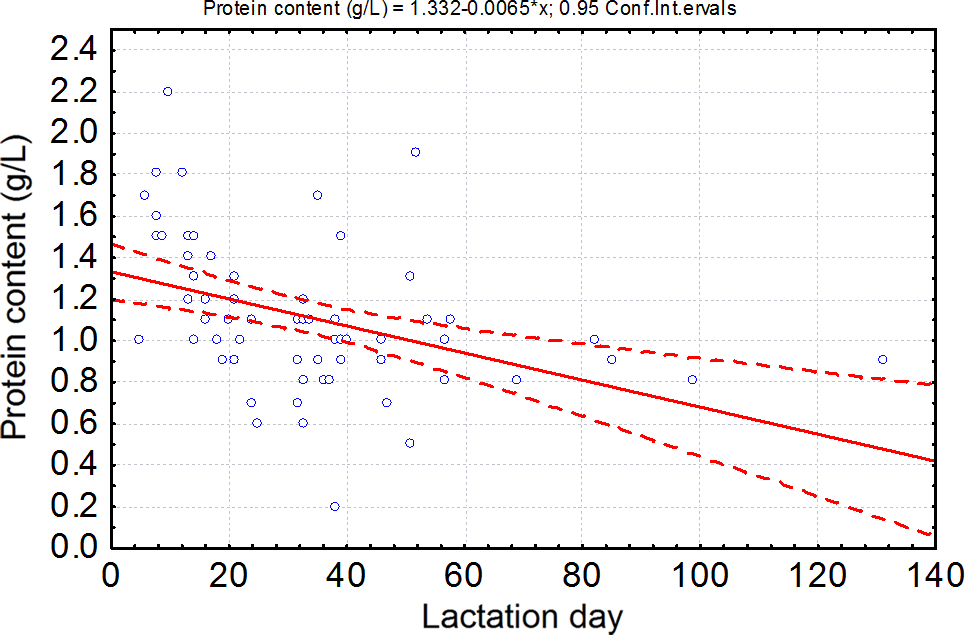
Protein concentration of milk expressed by mothers of preterm infants during the lactation period. We included 70 milk samples expressed by mothers of preterm infant between the 5th and the 131st day of lactation in the analysis.
This is one of the things making enteral nutrition with maternal breast milk difficult. Breast milk fed babies, as a group, grow more slowly than formula fed babies, often because some of them aren’t getting enough protein. As yet, breast milk fortification is standardized, but these types of variability really support the idea that individualized fortification might be preferable. Right now the difficulties with frequent breast milk analysis mean that a baby receiving breast milk and not growing adequately gets a blind increase in either feeding volume or fortifier; whereas they might benefit more from just a protein supplement for example.
Einloft PR, et al. Supplemented vs. unsupplemented human milk on bone mineralization in very low birth weight preterm infants: a randomized clinical trial. Osteoporosis International. 2015;26(9):2265-71. This trial in VLBW infants confirms that human milk fortifiers improve bone mineralization when they receive human milk. There is nowhere near enough phosphorus and not enough calcium in human milk for very preterm infants.
Omarsdottir S, et al. Cytomegalovirus infection and neonatal outcome in extremely preterm infants after freezing of maternal milk. Pediatr Infect Dis J. 2015;34(5):482-9. In a previous NICU we decided to routinely freeze all breast milk for preterm infants, because of lab evidence of CMV inactivation during freezing and thawing. In this RCT 140 infants were randomized to either have their mother’s milk frozen before it was fed to them, or to receive unfrozen milk. There was no overall difference in CMV transmission, many of the mothers produced CMV positive milk. When the analysis was restricted to those with CMV positive milk, the CMV transmission rate with CMV-DNA positive milk was 8% (3 of 37) in the intervention group and 6% (2 of 33) in controls. Freezing the breast milk reduced the rate of serious fungal infections however, which is possibly a true effect of the freezing, or perhaps a spurious result as they did make a large number of comparisons.
So let’s go back to the study from Corpeleijn, A secondary analysis of their data, that is, in essence, an observational study using their data showed that the infants who received more than 50% of their feeds as mother’s milk (which was supplied non-pasteurized) had many fewer infants with the primary outcome. 
The groups were diverging before 10 days of life.
It may be that unpasteurized maternal milk is the best source of milk for very preterm infants, with fewer infectious/NEC complications. But there will never be an RCT of maternal vs donor milk so we’ll just have to accept that, I think. The benefits of donor milk aren’t as clear, but there may be a reduction of NEC compared to the rates with formula, a reduction which isn’t evident if the comparison is just for 10 days. Human milk needs fortification to optimize bone mineralization, and composition is so variable that often extra fortification will be needed to get to optimal protein intakes. CMV transmission is very frequent and doesn’t seem to be prevented by freezing the milk; the importance of postnatal CMV transmission is something that has been studied recently in several investigations… there could well be a post about that!







Hi Keith,
I’m sure you are aware of the ongoing Milk trial in the NICHD NRN to evaluate the effects of donor milk vs formula on 2 yr outcomes (in addition to other outcomes): https://clinicaltrials.gov/ct2/show/NCT01534481?term=NCT01534481&rank=1
I was aware, but forgot about it when I was writing the post. Can you tell me what is being done with fortification? I presume cows milk based fortifiers will be used when the docs decide to enrich the milk, is that true?
Is there any research regarding fortification with Prolacta (a human milk based fortifier) vs HMF (a cow’s milk based fortifier)? We use both in our NICU – the Prolacta being so expensive is only used after proof of HMF intolerance (either NEC or bloody stools without pneumotosis). When we first received Prolacta every baby was placed on it – but within a year it fell into disfavor as the babies weren’t growing adequately.
Prolacta have only performed 2 tiny trials, which did not find a difference in their primary outcome. There was an enormous incidence of NEC in the controls, higher than I have ever seen, in the unblinded trial.
you can read about them here:
I would be interested to hear your thoughts on our recent growth and tolerance. The feedback we have gotten is that the growth was better than previously seen with donor milk. It can be found on our website at http://www.medolac.com
Our process deactivates CMV, and we are one of the few milk banks that screens the milk prior to processing ensuring the bacteria levels are within acceptable thresholds. Our pools of milk average 2,000 gallons at a time which allows the milk to reach mean nutrient content.
We encourage the use of a human milk analyzer since we see unbelievable variation in the nutrient content of mothers milk.
If there are gaps in milk bank products that the neonatology community would like addressed we are very responsive to this, and would love to hear it.
To know if one product or another really affects growth you would need to do a prospective comparative trial. On the other hand standardization of macronutrient intake with banked milk could easily make it less likely that one was giving low protein, or low calorie milk to a baby.
A human milk based fortifier, highly concentrated or powered, which has good enough research to prove efficacy, would be great. I would really want it to be very highly concentrated so that we don’t reduce the amount of mother’s own milk that we were giving.