
Since the death of Maureen Hack last week, I have been thinking a little about some of her important contributions to neonatology. In part because whenever I present, or write, about the prediction of outcomes in very preterm babies, I include a table from one of her publications. (Hack M, et al. Poor Predictive Validity of the Bayley Scales of Infant Development for Cognitive Function of Extremely Low Birth Weight Children at School Age. Pediatrics. 2005;116(2):333-41.)
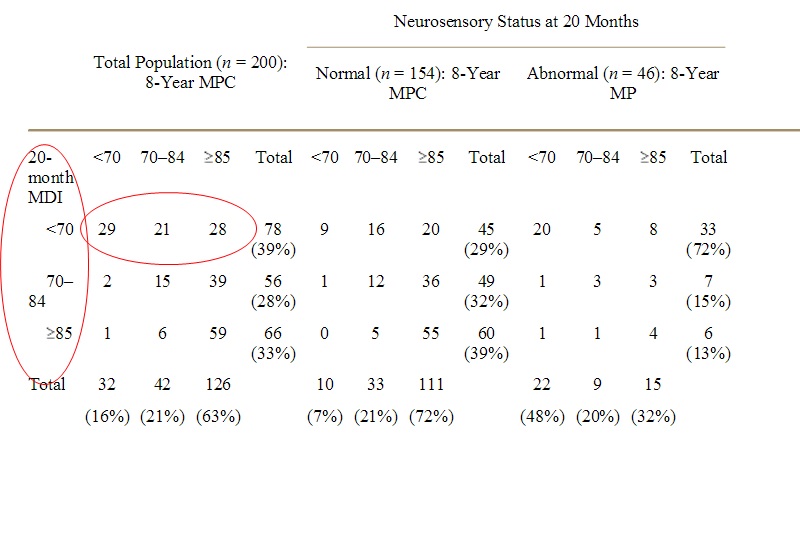 What Maureen and her team did was to compare the scores on the mental development Index (MDI) of the Bayley Scales of Infant Development version 2 at 20 months of age in a cohort of 200 very low birth weight babies, to the scores on the Mental Processing Composite (the MPC in the table) of the Kaufman Assessment Battery for Children performed at about 8 years of age. The MPC is a test of cognitive function. The Bayley MDI is often referred to as a test of cognitive function also, and children with a low score are often referred to as “cognitively impaired” which is a terminology which drives me bonkers as it is very inaccurate. As this table shows better than anything. Children with a 20 month Bayley MDI more than 2SD below the mean, that is less than 70, only 1/3 of the time had low scores on the MPC. The results also show that infants with neurological impairments and a low Bayley score were more likely to have a low MPC at 8 years than those without.
What Maureen and her team did was to compare the scores on the mental development Index (MDI) of the Bayley Scales of Infant Development version 2 at 20 months of age in a cohort of 200 very low birth weight babies, to the scores on the Mental Processing Composite (the MPC in the table) of the Kaufman Assessment Battery for Children performed at about 8 years of age. The MPC is a test of cognitive function. The Bayley MDI is often referred to as a test of cognitive function also, and children with a low score are often referred to as “cognitively impaired” which is a terminology which drives me bonkers as it is very inaccurate. As this table shows better than anything. Children with a 20 month Bayley MDI more than 2SD below the mean, that is less than 70, only 1/3 of the time had low scores on the MPC. The results also show that infants with neurological impairments and a low Bayley score were more likely to have a low MPC at 8 years than those without.
Very very few children (3) who were above that threshold at 20 months had poor cognitive function at 8 years. Which I think shows the real, limited, value of performing a Bayley at this age, as a test to identify infants who may need intervention, and conversely, those who will probably do just fine.
You can see the difference in the proportion of infants of VLBW who are defined as having a problem from the total percentages of low scores: at 20 months of age using the Bayley 2 MDI, 39% had low scores. At 8 years of age it is only 16%. Which has huge implications if you think that “cognitive impairment” is important, which I think most of us do.
Maureen was also one of a small group of investigators who have followed very premature babies out to adolescence and adulthood, and have also included a control group. One of the many striking publications from her cohort, born in 1977 to 1979, was this one, (Hack M, et al. Outcomes in young adulthood for very-low-birth-weight infants. The New England journal of medicine. 2002;346(3):149-57.) The VLBW subjects, were functioning very well in general, most having finished high school (66% of boys and 81% of girls) somewhat fewer than the controls (75% and 90%) and another 9% of the VLBW boys and 5% of girls were trying to get high school equivalency certificates. Many were in higher education, although fewer than the controls.
One of the things that I found most striking in her data, was the social deprivation of the group that Maureen was studying, one part of the evidence of that was the rate of incarceration of both the VLBW and the controls. 26% of each group had been in jail or youth detention at some point (including overnight). In addition VLBW boys were less likely to have actually broken a law, VLBW girls were less likely to be sexually active, and both sexes were less likely to have taken illegal drugs.
One of Maureen’s older studies that I think is still very pertinent is from 1989, (Hack M, et al. Differential effects of intrauterine and postnatal brain growth failure in infants of very low birth weight. American journal of diseases of children. 1989;143(1):63-8). She showed that VLBW infants who had postnatal growth failure, especially in terms of head growth, had substantially worse outcomes, and this was not necessarily the case for VLBW infants who were growth restricted at birth. Which points out the importance of good postnatal nutrition, aimed at ensuring good head growth.
Maureen and her group enrolled and studied another cohort, this time of extremely low birth weight infants (<1000g) born in 1992 to 1995.
Litt JS, et al. Academic achievement of adolescents born with extremely low birth weight. Acta Paediatr. 2012;101(12):1240-5. The average IQ in adolescence of the ELBW infants was 87, again the importance of a matched control group was demonstrated by this study, the controls had a mean IQ of 96. There were many more mathematics learning disabilities in the VLBW infants, and more executive function difficulties. Many more required special assistance at school. Hack M, et al. Self-Reported Adolescent Health Status of Extremely Low Birth Weight Children Born 1992-1995. Pediatrics. 2012. The overall self-reported health status of the ELBW adolescents was very similar to the controls. There was less risk-taking behaviour, and less physical activity, but overall they were doing well.
Finally (and I could do this for a while, but I am just picking out a few of what I think are highlights, there are many others that someone else might choose instead): Wilson-Costello D, et al. Improved Neurodevelopmental Outcomes for Extremely Low Birth Weight Infants in 2000-2002. Pediatrics. 2007;119(1):37-45. This study compared the 20 month outcomes of ELBW infants during 3 different time intervals, the 80’s, the 90’s, and 2000-2002. The survival improves progressively reaching 71% in the 3rd period. Neurodevelopmental outcomes improved also, the “neurodevelopmental impairment” was lowest in the latest cohort.
I have decided that from now I on refuse to use that term. I will call it neurological impairment and developmental delay, NIDD.
In this publication, the rate of NIDD fell from 35% to 23%, developmental delay did not change much, the MDI scores were similar, but there was less cerebral palsy and less deafness and blindness. The study didn’t use the GMFCS system, but states that they only included moderate and severe CP. I think using the term impairment for CP, deafness and blindness is appropriate, (although including hypertonia and hypotonia might inflate the numbers a bit) they tend to persist, although the diagnosis of CP might occasionally change, and they satisfy WHO definitions of “impairment”. Low Bayley scores are not an impairment, overall 2/3 of the infants will not be impaired on later cognitive testing, as Maureen showed.
The largest component of the NIDD is low Bayley scores, 21 of the 36 infants with NIDD in this study met the definition because of a low MDI. We can therefore estimate how many will still be considered impaired at 8 years of age. As I noted above, infants with a low Bayley score who did not have a neurological impairment were more likely to have higher scores on the 8 year MPC. Only 9 of the 45 infants with a Bayley2 MDI less than 70 but who did not have a neurological abnormality had an MPC of under 70 in the 2005 article from Pediatrics at the top of this post, and could be considered to have a cognitive impairment. If that still holds true (and there is other evidence that it does) then the total frequency of neurological or cognitive impairment of this group at 8 years will be about 12%.
How can we further reduce this proportion? Maureen also studied the impacts of sepsis, of necrotizing enterocolitis, of postnatal steroids, and of bronchopulmonary dysplasia, and confirmed their negative impacts on outcomes. Reducing the incidence of those complications, and improving postnatal nutrition and growth will reduce their negative effects on NIDD, and eventually on NCI.
Thank you Maureen, farewell.






