Current guidelines support the use of therapeutic hypothermia for term infants with hypoxic ischaemic encephalopathy. Both the Canadian and the US guidelines include infants born at 35 weeks gestation. However, the data supporting efficacy for those late preterm infants, is extremely limited, and less mature infants were excluded from all the major trials. The discussion section of this new publication reveals that the 2 RCTs which included babies of 35 weeks GA had a total n of 7.
The primary outcome was death or disability, with disability defined as severe : Bayley III cognitive score <70, GMFCS level 3-5, blindness, or deafness despite amplification; or moderate : cognitive score 70-84 or, GMFCS level 2, treated seizure disorder, or hearing loss requiring amplification. Primary analysis was a Bayesian approach, with the prior assumption being no effect of the intervention.
As you can see there was no indication of any benefit. Death was more frequent in the hypothermia group, and outcomes among survivors were just about identical, a slightly proportion with severe disability in the hypothermia group (and interestingly, almost no survivors with moderate disability, in either group, 2 vs 0). The Bayesian analysis shows there is very low probability of benefit of cooling in this population. Also, there were many of the cooled babies who overshot their target, 32 of them had a temperature recorded under 320 during the first hour of intervention.
Interestingly, the way this is presented in the table is that there is only a 13% chance of benefit on mortality with cooling; in the discussion this is stated as an 87% probability of harm from the treatment, which gives a zero chance that the treatments are equivalent! Maybe it’s just my poor understanding of Bayesian analysis. Within Bayesian analysis there are ways of evaluating different magnitudes of treatment effect, which is something that I think we should consider for the future, rather than presenting data as if the only 2 possibilities are that the outcomes are either better or worse, it would perhaps be more helpful to calculate the probabilities of a particular, clinically important impact, and the probability that mortality is about the same, using whatever limits are considered appropriate. I guess, if the probability of benefit had been about 50%, then you could say the treatments are equivalent?
On the other hand, for this intervention, as there is very low probability that cooling is beneficial, we should not cool the late preterm infant with encephalopathy. For babies at 35 weeks, these data are much stronger than those previously available, and 35 week GA infants should probably not be offered therapeutic hypothermia, and should be excluded from the next version of any guidelines.
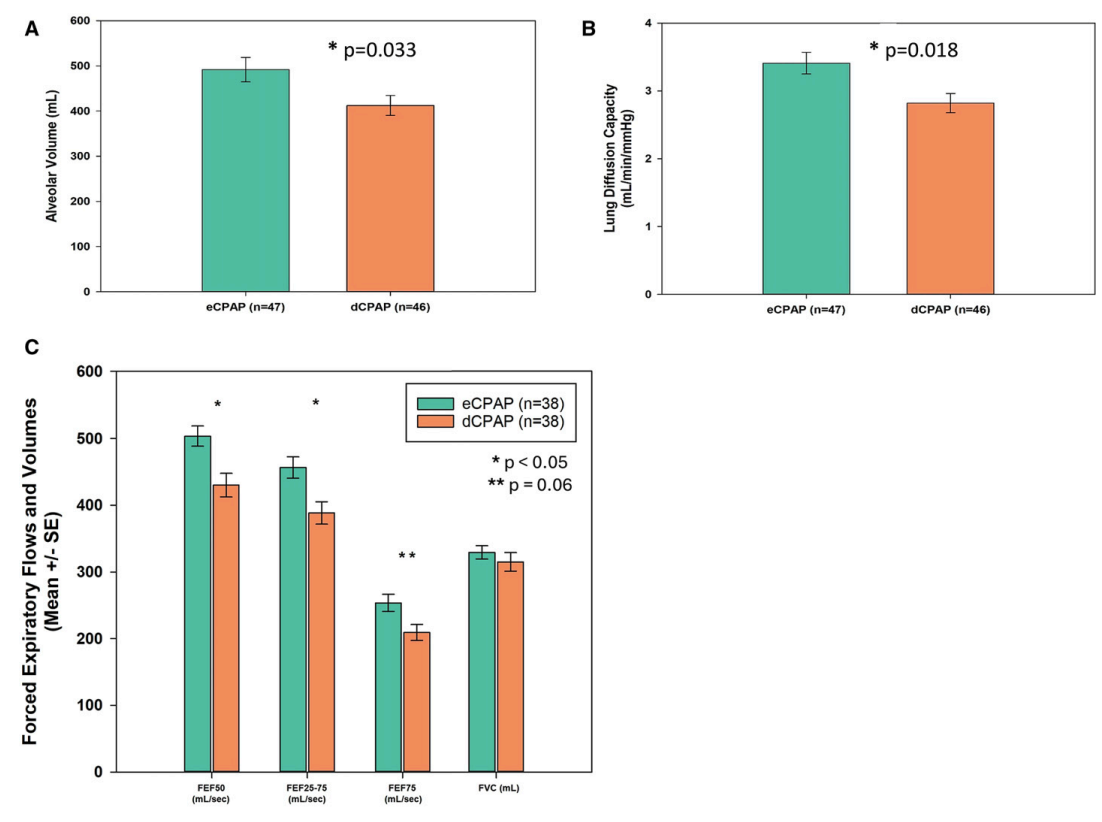
The trial enrolled 100 preterm infants (24 to 32 weeks GA) who had at least 24 hours of CPAP and were considered ready to have the CPAP stopped (5 cmH2O, 21% O2, without tachypnoea or retractions or frequent apnoea, and tolerating breaks from CPAP during care procedures). They had to satisfy these criteria for 12 hours to be considered “stable”. (The pilot trial published previously used a pressure of 4-5 cmH2O, with the same criteria). They randomized the babies to their usual care, which was stopping the CPAP, or to remain on CPAP for a further 2 weeks. Neither this publication, nor the pilot, nor the registration documents, states what pressure was used for this extended CPAP treatment. Which I think is critical, did they use 4 or 8 cmH2O? or something in between?
Babies averaged about 30 weeks GA, and were eligible for the trial at a mean 32.4 weeks PMA, a minority in each group had required surfactant (25% vs 37%). Occasional infants paused the extended CPAP because of local nasal trauma, and occasional controls had to have their CPAP restarted.
Short term results confirmed the increase in FRC with prolonged CPAP, as demonstrated in the pilot, when measured just after the intervention period. At 6 months the infants had lung function testing, which showed improved Alveolar volume, improved DLCO, and better Forced Expiratory Flows.
FEF is, of course, a measure of small airways function, and is frequently impacted by preterm delivery, this result is reassuring that the increase in alveolar volume is not just because the alveoli are distended, but probably lung growth overall is increased, including small airways. That would be consistent with findings from animal models; prolonged CPAP does not simply distend the lungs, it seems to promote lung growth, and, in a couple of models, decreases airway reactivity.
Parents were questioned about wheezing, and bronchodilator use. The questionnaire also asked about hospitalisations, and respiratory hospitalisations, but those data are not reported. Babies in the extended CPAP group were less likely to have wheeze, 43% vs 56%, but this is within the confidence intervals of no difference.
The major limitation of this trial, in terms of impact on clinical practice, is that these are babies with very little lung disease, only about 7% in each group had BPD, (Oxygen at 36 weeks). Although even such relatively minor lung disease of prematurity is known to lead to long term impacts on pulmonary health, whether the intervention would be equally as effective among infants with sicker lungs is unknown.
Routinely extending every baby’s CPAP by 2 weeks would have major impacts on resource utilisation, so we really need robust data. It also could have adverse impacts on oral feeding, especially breast feeding, during the time period when orality is also developing. Most of the babies in this study finished the intervention between 34 and 35 weeks, so the interference with developing breast feeding may have been small, but if babies who become eligible later (in terms of PMA) are treated with extended CPAP, the progression of breast feeding might be a major issue.
I hope that further trials, including infants requiring oxygen supplementation, and with more extensive analysis of outcomes of direct interest to parents, are planned. I also hope that the possible impact on breast feeding is investigated. If every very preterm baby, who is otherwise clinically ready to have their CPAP discontinued, will have that treatment extended for 2 weeks, we need to be very sure that the benefits justify the extra resources, and that there are no balancing negative effects.
I used to do a series of shorter posts called “weekly updates” but I ran out of steam and have concentrated on longer posts in recent years. The last couple of weeks, with clinical service, I have had less time for a longer post, but a few things piqued my attention:
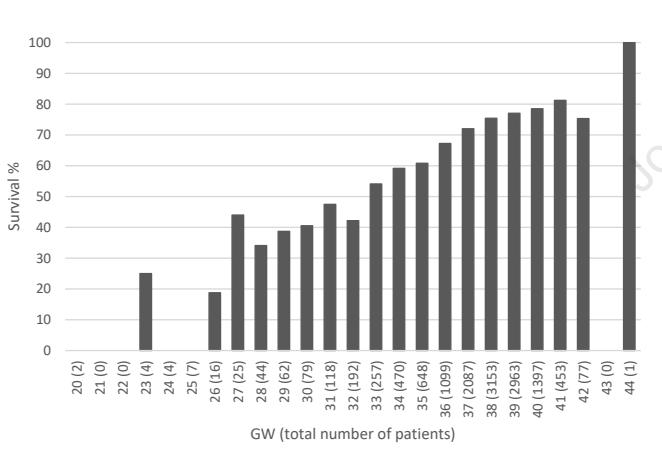
There was also an article about congenial cataracts, and several others about congenial heart disease. The pre-print of the article has the error right on its front page, it has probably been seen by hundreds of pairs of eyes, and everyone’s brain auto-re-corrected it back to congenital! I am not writing about this just to poke fun, however, it really is a very interesting piece of work from an international consortium, reporting analysis of over 13000 cases. It demonstrates very clearly the major impact of prematurity on management and outcomes of CDH. Survival of all cases progressively increases up to 40 weeks gestation.
For infants of <34 weeks gestation, large numbers never have a surgical repair, nearly half, and those that do, get their surgery much later, at 11 days mean, compared to about 1 week for the early term and term groups. ECMO was used in about a third of the cases after 34 weeks, but only 7% of the <34 week infants. ECMO survival was 30% for the <34 weeks, 40% for the late preterm, and just over 50% for the term infants. All of the measures were more marked for the very preterm, and worse again for the extremely preterm.
Within the database there are many infants who delivered after fetal intervention (FETO), which was associated with lower survival. This was clearly because they were a much higher risk group, which is why they were selected for FETO, overall survival was only 54% after FETO, compared to 71% among the remaining infants, and almost all of the FETO babies needed a patch repair. FETO was also associated with increased prematurity, and among those who did deliver preterm, survival was poor, about 40%, but was identical with or without a prior FETO.
Take Home Message : Prematurity is very bad news for infants with CDH.
Franz AR, et al. Effects of liberal versus restrictive transfusion strategies on intermittent hypoxaemia in extremely low birthweight infants: secondary analyses of the ETTNO randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2025. This is a secondary analysis of the ETTNO trial, the primary publication of which which showed no overall benefit of a higher versus a lower transfusion threshold in the very preterm infant. This analysis focused on any potential impact of transfusion threshold on apnoea spells, which are the usual pathophysiology behind intermittent hypoxia. Multichannel recording and analysis of apnoea patterns, which I have done, and published, many hundreds of times and published is much more difficult and time consuming than just recording oximeter saturation data. In addition, unless you record airflow as well as just respiratory movement and heart rate, you gain very little, and measuring airflow is tricky. Most recent studies therefore have measured, and discuss, intermittent hypoxia.
I actually started an RCT of transfusion therapy for apnoea when I was in San Diego, we enrolled only about 20 patients prior to me leaving UCSD, and the fellow also graduated, so the trial ground to a halt unfortunately. I did have a poster at an SPR about our preliminary findings, but never felt that it was worth a publication. Basically we performed multi-channel recordings, including an expired CO2 detector next to the nose of the infants, among convalescent preterm babies with apnoea and a hemoglobin <100. We randomized them to get an immediate transfusion if the attending physician thought it was reasonable to transfuse, or to not be transfused for at least 72 hours, and did physiological recordings for 72 hours. The trial was of course therefore very underpowered, but there was no impact of transfusion on the respiratory patterns of the babies.
We did that trial because, at the time, recurrent apnoeic spells were often as an indication for transfusion in anaemic preterm infants. There were also a few observational cohorts, which suggested that apnoea becane less frequent after transfusion, but those cohorts were all uncontrolled. Control groups are essential for many things, but especially with a condition such as apnoea of prematurity, which always gets better with time anyway! Without a control group, any intervention that you can imagine will be followed by decreased apnoea, especially when you factor in that babies are usually enrolled in a trial when their apnoea frequency is at its highest. I was rather sceptical about apnoea as a transfusion indication, which was the justification for the RCT.
This new publication has compared intermittent hypoxia episodes, occurring between days 8 and 49, between infants in the higher transfusion threshold group to the lower group. All the babies were less than 1kg, and there were over 250 per group.
There was no difference between the groups in numbers of IH episodes, duration of episodes, more severe episodes, or the median duration of episodes. Or indeed, as they have previously published, on survival or neurological or developmental outcomes. There was also no interaction between IH, transfusion strategy, and outcomes.
Take Home Message : Intermittent hypoxia, and/or apnoea of prematurity is not an indication for blood transfusion.
Cheung PY, et al. Dose-related systemic and cerebral hemodynamic effects of norepinephrine in newborn piglets with hypoxia-reoxygenation. Pediatr Res. 2025. Po-Yin Cheung and the group in Edmonton refer to the lab where they do their animal work, as my old lab; I set up many of the processes and bought some of the equipment that they are still using 30 years later, including the Transonic flow probes! Po-Yin, and Georg Schmolzer, and their colleagues, have gone far beyond what little I accomplished there, however. This new publication is in acutely instrumented anesthetised newborn piglets, and investigates the haemodynamic and cerebral circulatory effects of norepinephrine infusions. The model they use is one developed by Po-Yin, of hypoxia and re-oxygenation, and is designed to be a model of infants after perinatal asphyxia.
Our group in Montreal have been using norepinephrine for circulatory support for a few years now, mostly for septic shock or for infants with PPHN who need support. In both circumstances there is a small amount of animal data, and a very small amount of human neonatal data suggesting advantages over other agents. One thing that has been missing is a good idea of what the agent does to the cerebral circulation, being very difficult to accurately measure cerebral perfusion in the newborn infant.
The model used in this study leads to a severe metabolic acidosis, lactate of 20 and Base Deficit of 20, and 2 hours later, prior to the study medications begin administered, the acidosis was a little improved. Animals then got either saline, or epinephrine infusion at 0.1 mcg/kg/min or one of 3 doses of NorEpinephrine (0.05, 0.1 or 0.2 mcg/kg/min). Without going to all the details of the findings, NE at 0.1 mcg/kg/min had the biggest positive impact on cardiac function and cardiac output, With cardiac output increasing by 100%, due to a small increase in heart rate, of about 20%, and a major increase in stroke volume. At the same time systemic blood pressure increased by about 20%.
In addition carotid blood flow increased by nearly 20% leading to an increase in cerebral oxygen delivery and brain oxygenation.
Clearly, one cannot directly extrapolate these results to the human newborn, and particularly not specific dose responses, but they do give some reassurance that norepinephrine does not vasoconstrict the neonatal cerebral circulation.
Take Home Message: (with lots of caveats) norepinephrine infusions may lead to improved cerebral oxygenation.
Fox L, et al. A Pilot Randomized Control Trial of Holding During Hypothermia and Effects on Maternal and Infant Salivary Cortisol Levels. Adv Neonatal Care. 2025;25(2):173-80. Many centres, including ours, have instituted “cool cuddles” (câlins-frisquets in Quebecois), whereby infants with HIE being cooled are allowed to be cuddled by their mothers (or fathers!). We have demonstrated, for our own purposes, that this doesn’t adversely impact temperature control. We still have a few restrictions, for infants with multiple central lines it gets quite difficult to ensure safety. Although it seems like the right thing to do, from first principles, this new randomized trial sought signs of infant stability and stress, and maternal stress from their salivary cortisol levels. Mothers in the cuddling group had lowered cortisol, as did their infants, who also showed lower, stable heart rate and respiratory rate, without desaturation, or temperature problems.
Take Home Message : Cuddling during therapeutic hypothermia reduces maternal stress.
A few years ago, we published our experience with the use of hydrocortisone in newborn infants in septic shock (Altit G, et al. Corticosteroid Therapy in Neonatal Septic Shock-Do We Prevent Death? Am J Perinatol. 2018;35(2):146-51), like many such studies the numbers were small, but the 39 babies who received hydrocortisone in addition to their inotropic support had rapid haemodynamic improvement, within 6 hours of starting hydrocortisone, mean BP had increased by over 30%, urine output was better, and inotropic support was being weaned. They were, however, somewhat less likely to survive the episode (59% survival vs 78% without hydrocortisone) and to survive until discharge, neither of which comparisons were “statistically significant”, and the babies who got hydrocortisone were sicker, less mature and more likely to have NEC, than the septic babies who did not get hydrocortisone.
Those data suggested that there was a major rapid haemodynamic response to hydrocortisone in newborn infants with septic shock, but they clearly could not answer the important question about whether they improved survival.
A new, single-centre prospectively-registered RCT has examined this issue. (Dudeja S, et al. Early hydrocortisone verses placebo in neonatal shock- a double blind Randomized controlled trial. J Perinatol. 2025). Newborn infants with shock, of any aetiology, were enrolled in 2017 and 2018 (not clear why the delay in publishing) and randomised to receive early hydrocortisone, or placebo. It is also not clear why they bothered with the placebo, as the bedside nurse was not masked to study group assignment. The main problem with the trial is the definition of shock, which was either A or B criteria “(A) either systolic or diastolic blood pressure (BP) less than 5th centile; (B) Any two of the following five criteria- capillary refill time >4sec, core-periphery temperature difference >3 °C, urine output <0.5mL/kg/hr in previous 6 h, base excess worse than −5.0mmol/L and lactate >5mmol/L”.
The use of BP alone to define shock is problematic, at any moment 5% of healthy babies are below the 5th percentile, and therefore over 5% of all babies are in shock at any time according to this definition. In addition, the definition allows cuff, non-invasive, BP to be used, which are very unreliable, and they used standards for BP which are limited (Zubrow AB, et al. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. Philadelphia Neonatal Blood Pressure Study Group. J Perinatol. 1995;15(6):470-9). Many infants had a large PDA, which will lead to low diastolic pressures satisfying this definition, but without necessarily having other features of shock. Nevertheless, these were babies that the clinicians felt warranted vasopressor/inotrope intervention. To be eligible for the trial the infants had to be “fluid-resistant”, that is not responding to 1 to 2 10 mL/kg fluid boluses, they also excluded infants with NEC, I am unsure why.
Infants were started on vaso-active drugs at the same time as the study drug, and had functional cardiac echography. The primary outcome was survival to 14 days of age, rescue hydrocortisone was allowed if the infant became unresponsive to their vaso-active drugs.
Survival was very poor in both groups, 17% with placebo, and 28% with early hydrocortisone. and 80% of the controls eventually received open label hydrocortisone (compared to 70% of the early HC group).
There are a couple of reasons for this post, the first being that I think this is the first report of an RCT of steroid use in the treatment of circulatory collapse in the newborn, which points out how poor the evidence is to support anything that we do. And also because the survival is reported just as being “not significant”. I mentioned Bayesian analysis in a previous post, and I think that a small trial such as this, which was very unlikely to have a “statistically significant” result, because of low power, is nevertheless informative, and is a good candidate for Bayesian analysis. Using an on-line Bayesian calculator, it seems that likelihood that the early hydrocortisone group is better is about 88% (I am certainly no expert in these calculations, and I may be in error!)
Another way of presenting these results is with the relative risk and its confidence intervals, which is 0.87, 95% CI 0.69 – 1.10. Which means that the results are consistent, with that level of confidence, with no difference in mortality, a small increase in mortality, and a major decrease of 31% in mortality.
The implication of this is that there is certainly enough suggestion of a substantial benefit that further trials are warranted.
I am not against publishing such small trials, I think they can give valuable pointers for the future, but we should be very careful how the results are presented. The abstract of this article just states “we did not observe a significant reduction in 14-day mortality”, which is actually misleading. It would be more accurate to state “we observed a major reduction in mortality with early HC use, but it was not statistically significant, and may have been due to chance effects in a small underpowered trial”. Maybe we should ban the use of the word “significant” from the medical literature. It is often used, as in this abstract, to mean “statistically significant”, but is often interpreted as “real”, “meaningful”, or “important”.
I can’t remember is I participated in this questionnaire, but, if I had, I would be one of the “other” group! I don’t give fluid boluses for hypotension, unless I have good reason to suppose that the infant is hypovolemic. Early hypotension in the preterm is now much less common, because of delayed cord clamping, and is almost never due to hypovolemia. I will sometimes giving a fluid bolus in shock, if I think that the baby needs more preload, and I tend to start HC very early when I feel that vasopressor/inotrope therapy is needed. In suspected septic shock, for example, I will usually start HC at the same time as the norepinephrine. I have no idea if that is the right thing to do, but 100% of the respondents to the survey reported using HC for hypotensive babies, at least some of the time.
There is clearly a need for further trials; the question of timing of HC use in babies with shock is clearly very important, and could have an important impact on mortality.
When the platypus was first captured, killed, skinned and the pelt sent to a zoologist in London, George Shaw in 1799, he thought he was being scammed. He tried to find the stitches that had been used to cobble together the specimen. Being unable to do so, he then concluded that it was probably real, and was unique. It was what we would now consider an evolutionary innovation, it had features of previous organisms, such as laying eggs, and several new features, being venomous and producing milk to feed their young, once they have hatched. Here is a photo I took in March 2023 at the Woonoowooran national park.
Adaptive designs first went mainstream during the COVID epidemic, with the dramatically effective RECOVERY platform. The trials were able to be launched, and to rapidly provide clinically vital results within a very short period of time, while the pandemic was still at its height. RECOVERY was able to rapidly prove the value of standard dose steroid treatment for improving outcomes, and then showed that higher dose dexamethasone was a bad idea, and should not be used. They have also shown that some antivirals are ineffective, that routine azithromycin made no difference, and have to this point enrolled nearly 50,000 patients, having now expanded to find treatments for complicated influenza and non-viral community acquired pneumonia.
Another platform design has, just this last week, produced some important results in ALS, also known as Lou Gehrig’s disease in the USA, and Motor Neurone Disease in the UK. There are 4 simultaneous comparisons published, with 3 different interventions compared to a common control group. None of the interventions showed a clear benefit, but there were some suggestions of some improvements, which allows, within the platform design, to proceed rapidly to adjusted protocols, perhaps in subgroups. An editorial article accompanying the publications discusses the limitations, and the major advantages of such trials. In ALS, the Healey platform was funded by, and named after, a very wealthy man who has the condition himself.
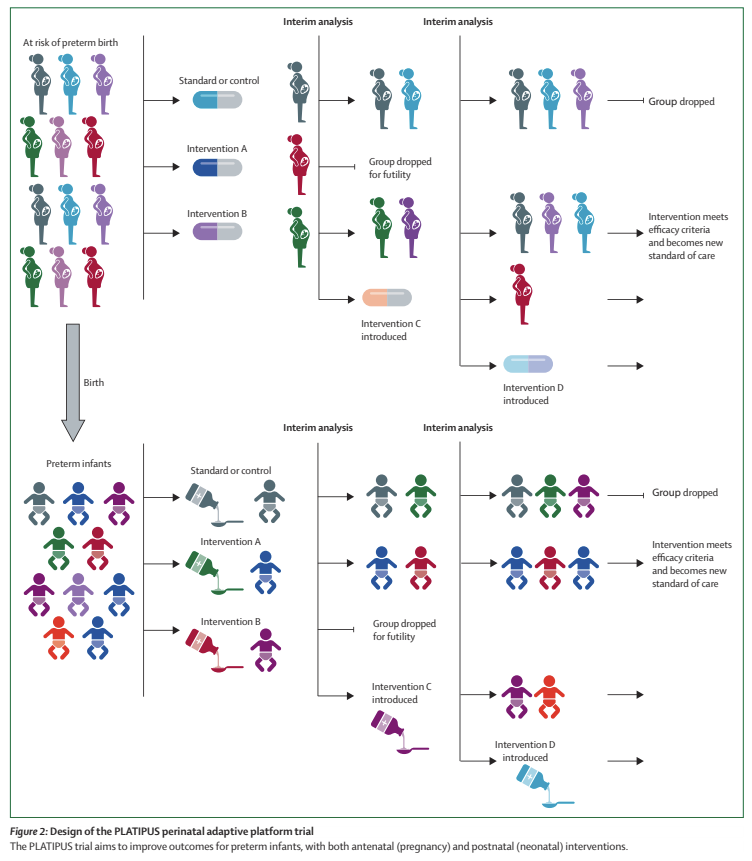
The first comparisons being investigated by PLATIPUS are, for the maternal domain, different antibiotic regimens for preterm PROM, with 3 different regimens being investigated. I must say I thought this was relatively settled, among the antibiotics in the trial, and that it was already fairly clear that azithromycin plus amoxycillin was the way to go, but it seems there is still some doubt about their relative efficacy, and the platform will allow the future investigation of other regimes with minimal adjustment. For the neonatal domain of the platform, they are investigating 3 different dosage regimes of caffeine, the standard dose that we used in the CAP trial, (20 mg/kg of caffeine citrate load, then 10 mg/kg/d, which they call the low-dose group) to a medium dose group which is 50% higher, and a high dose group which is double the standard dose.
The figure below is a schematic of how it might proceed.
The other part of the innovative nature of this trial is the outcome measure that is being used, which is an ordinal composite adjudicated at 42 weeks PMA. The outcome is scored from 1 to 15, with 15 being the worst outcome, death. Levels 1 to 15 are described as follows:
1= Well, liveborn infant; 2= Neonatal unit admission for <48 hours; 3= Neonatal unit admission for >/= 48 hours; 4= Non-invasive respiratory support or oxygen therapy for ≥ 4 hours & < 5 days; 5= Non-invasive respiratory support or oxygen therapy >/= 5 days; 6= Mechanical ventilation via endotracheal tube for ≥ 4 hours & <7 days; 7= Mechanical ventilation via endotracheal tube for >/=7 days; 8= Moderate respiratory morbidity; 9=Necrotising enterocolitis AND/OR Sepsis; 10= Severe Respiratory Morbidity; 11= Major Surgery; 12= Brain Injury; 13= TWO of severe respiratory morbidity OR major surgery OR brain injury; 14= Severe respiratory morbidity & major surgery & brain injury; 15 = Death
There is obviously a lot to pick apart and discuss here, but my first response is Bravo!! At last a composite outcome in a neonatal trial that recognizes that all competing outcomes do not have the same value! The definitions of each of these outcomes are on the clinicaltrials.gov website. For example “severe respiratory morbidity” is respiratory support at 40 weeks PMA, or discharge home on oxygen or respiratory support. Which seems to me to be a definition which is both consistent with parental concerns and reasonably predictive of longer term respiratory outcomes.
As for Brain Injury, I have a few more concerns, the definition given is : Major intraventricular haemorrhage, unilateral or bilateral, defined as i. Papile Grade 3 or 4 AND/OR ii. Moderate-severe periventricular haemorrhagic infarction b. Cystic periventricular leukomalacia, unilateral or bilateral c. Moderate or severe white matter injury on MRI at near-term or term equivalent age d. Any cerebellar haemorrhage e. Other major ischaemic injury such as arterial stroke or hypoxic ischaemic injury f. Post haemorrhagic hydrocephalus requiring drainage.
The problems with this part of the outcome are 1. using the Papile classification 2. including “any” cerebellar haemorrhage. 3. White matter injury on the MRI.
For this particular part of the composite outcome, I am not sure how much this matters, but if the high-dose caffeine group, for example, had more cerebellar haemorrhages, but less severe respiratory morbidity, then that group would be considered to be worse off, even if the haemorrhages were all tiny and had no long term impact. However, I am not sure if you could really tease all that out as part of an ordinal composite like this one, if there is a difference in brain injury, as defined in the protocol, between groups, that would probably be a reason for choosing between interventions, even if some of the haemorrhages had little long term impact.
For an adaptive platform trial trial like this the outcomes have to be determined rapidly after the intervention; 2 year neurological/developmental outcomes, or other long term outcomes of interest to parents cannot be the primary. Hopefully, all the infants randomized in the platform will have longer term outcomes evaluated and reported in addition to the primary short term outcome. I’m sure you are all aware that caffeine therapy in the CAP trial did have some minor short term benefits (infants came out of oxygen a little faster, so were less likely to be diagnosed with BPD, and less likely to have treatment for a PDA), but substantial, very long lasting benefits on follow-up.
Analysis of the trial results is also a major issue, the RECOVERY trials have used a fairly standard frequentist approach, with the first results showing advantages of standard dose dexamethasone being presented as the proportion of deaths in each group, the relative risk (0.83) and confidence intervals (0.75 to 0.93) and the p-value P<0.001. Platipus is planned with a Bayesian approach, which is less familiar to many clinicians, but has potential advantages. The Bayesian approach clarifies that no RCT really proves that one approach is better than another, which is suggested by our dichotomous “significant or not significant” current typical presentation of results, but gives an estimate of how likely it is that one intervention is better than another.
The Platipus platform will allow on-going adjustments, other comparisons, addition of other groups, and other interventions. It could become the default model for future trials in perinatal medicine, and should enable us to get results much faster, but just as reliably.
Platipus, just like the Platypus, will give us major scientific insights for the future. It should allow us to advance the care of newborns more rapidly than in the past.
Several trials of liberal versus more restrictive transfusion practices have been published, and overall, it seems that being very restrictive in transfusions has no negative impacts on clinical outcomes, and depending on the trial, some positive benefits of avoiding transfusion.
One of the important studies of the Canadian Critical Care Trials Group was the TRICC trial, which enrolled critically ill adults with a hemoglobin less than 9 g/dl, who were randomized to a target hemoglobin of 7-9 vs 10-12 g/dl. In that trial the adults with the lower target did better, with a lower in-hospital mortality of 22%, vs 28% with more liberal transfusion. In the results of that trial there was a suggestion of a different outcome in the subgroup with myocardial ischemia, so the group did another analysis in adults with cardiovascular disease, which showed no big differences in outcome, but still suggested a possible benefit of higher hemoglobin in those with unstable angina or an acute MI. Other studies have still, as far as I can see, not clearly answered the question in this subgroup of adults, and the most recent systematic review that I found basically stated “we don’t know”. As a result further trials are planned.
It could be that in patients with coronary artery disease, the ability to vasodilate and maintain myocardial oxygen delivery in the face of anaemia is limited, hence it is physiologically feasible that this subgroup would have different outcomes to those without serious coronary artery disease.
The same might be true for another subgroup, under-represented in the original TRICC and other trials, those with acute neurological injury. In this new trial in JAMA, adults with either traumatic brain injury, or a sub-arachnoid haemorrhage, or an intra-cerebral haemorrhage, who had a haemoglobin <9 g/dl, were randomized to a target of maintaining haemoglobin >9 compared to >7.
The rationale being that these groups of adults have a limited ability to increase brain perfusion in response to anaemia, and may benefit from higher haemoglobin, and that the previous studies have included very few such patients, and have also not measured longer term functional outcomes. The primary outcome of this trial was the extended Glasgow Outcome Scale after 6 months. We used a paediatric version of this scale in our recent publication (Boutillier B, et al. Survival and Long-Term Outcomes of Children Who Survived after End-of-Life Decisions in a Neonatal Intensive Care Unit. J Pediatr. 2023;259:113422. as it is a scale of functional capacities, in our study it was used in a descriptive fashion. In the new trial it was dichotomised into bad outcomes (1 to 5, 1 being death) and acceptable outcomes (6 to 8). The following table describes those scores
I will restrain myself from one of my usual rants about it being inappropriate to dichotomize continuous outcomes just for the simplicity of research design, or of equating death with being unable to use public transport! Designing and analyzing the trial using the GOS-E as an ordinal outcome would have been entirely possible.
800 patients, mostly in Europe and South America, were randomized, and outcomes were better in the higher hemoglobin group. The median GOS-E in both groups was 4, in other words large numbers of the patients had quite poor outcomes. As you can see from the graphical abstract above, the proportion with scores <6 was lower, 63%, with the higher HgB threshold compared to the higher threshold, 73%. When analyzed using an outcome of GOS-E<5, the higher HgB group still had an advantage, 50% vs 60%.
Why am I discussing this adult trial? I guess it is the first evidence, that I know of, that a higher hemoglobin threshold in critically ill patients improves outcomes. And that, in this group of patients we may have found the lower limit of acceptable HgB.
One thing we do not know in preterm babies is the extent to which they are able to vasodilate the cerebral circulation in the face of anaemia to maintain cerebral oxygen delivery. I guess this is why the people who designed the protocols that have been tested in neonatal transfusion trials have all used different thresholds during the first days after birth compared to later life. Or maybe it was just completely arbitrary!
The neonatal trials which have been published, which I have discussed previously used the following transfusion thresholds (converted to Hemoglobin in g/100mL).
The definition of “sick” varied between the trials. In none of the trials was there any sign of harm from the lower transfusion threshold.
I think we are therefore probably well above the threshold of harm, but the new trial does show that under certain circumstances a higher threshold may be better, and that, at least in adults with acute brain injury, a higher threshold may improve outcomes.
Might this be true in preterm infants? I’m not sure if there has been any subgroup analysis of infants in the RCTs who had a brain injury, obviously the pathophysiology of such injuries is dramatically different in preterm infants than the adults in the new JAMA RCT, and the physiology of the control of cerebral perfusion is different also. But those results do suggest that we should consider the possibility that there is a lower limit to transfusion thresholds, which may differ among different groups of babies.
We have known for a very long time that bilirubin can cause an encephalopathy leading to acute and chronic clinical impacts, the most severe chronic impacts being kernicterus, a disabling movement disorder and nerve deafness. What seems to be the case is that bilirubin bound to albumin doesn’t cross the blood-brain barrier, and that the BBB, which appears to develop early, and be functional by 20 weeks, is easily disrupted in the newborn. Bilirubin staining of the basal ganglia has been shown on autopsy specimens at much lower concentrations than are associated with kernicterus in term babies. This finding led to the performance of the large multicentre NICHD network phototherapy trial, which is very limited by the lack of a funky acronym. Can I suggest that we start calling it the “LITEPOP” trial: Longterm ImpacTs of Early Phototherapy for Outcomes of Preterms?
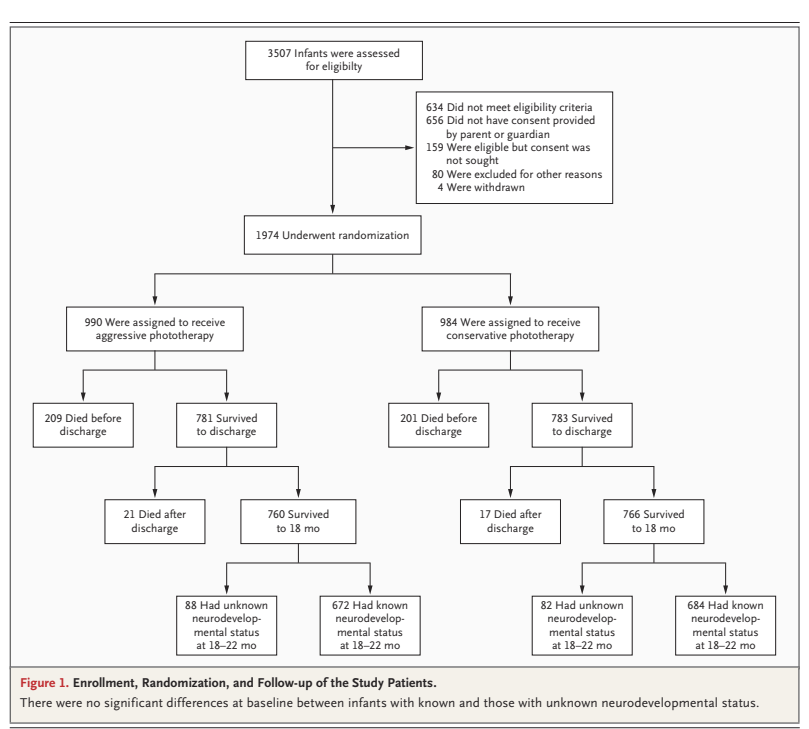
There have been multiple studies looking at “free” or “unbound” bilirubin and its impacts, which are hindered to some extent in difficulties measuring it. The subject of this post is a new re-analysis of data from that NICHD early phototherapy LITEPOP trial, which finished enrolling in 2005, and finished follow up 2 years later, with the primary publication (Morris BH, et al. Aggressive vs. conservative phototherapy for infants with extremely low birth weight. N Engl J Med. 2008;359(18):1885-96) appearing in 2008. If you remember, or if you have never heard about this, the primary outcome was “death or NDI” (groan…). There were nearly 2000 babies of 501 to 1000 g bwt randomized at 12 to 36 hours of age if they had never had phototherapy. The intervention was to have phototherapy started immediately and continued until it fell below 85 micromol/L (5 in the US units). The control group had phototherapy to keep the bilirubin either below 137 (500-750 g bwt) or below 170 (751-1000 g).
The results are a very apposite demonstration of the problems with such a composite outcome. Mortality was just about equal in the two groups, 209 vs 201 died before discharge, and a further 17 vs 21 died after discharge, or 24 vs 23% total mortality.
The NDI data were presented as among the entire groups (survivors tested plus deaths), i.e. 235/902 vs 275/902, which is statistically significant, 26% vs 30%, (RR 0.86 (95% CI 0.74–0.99)) but because of the 1% higher mortality in the early phototherapy group, the combined outcome of “NDI or death” was not considered significant.
If we recalculate the outcome of “NDI” just among the survivors who were tested, 235/672 vs 275/684, 35% vs 40%, and the proportion with low PDI scores 127/672 vs 152/684, 19% vs 22%, or with severe hearing loss, 9 infants vs 28, or with athetosis, 2 infants vs 10, then the differences all suggest benefit of early phototherapy.
Babies in this study had a blood sample stored at 5 days of age, which was later measured at one of 2 laboratories. Although they used the same method, (the peroxidase method) and the same analyser, there were enough differences between the 2 labs that the results were converted to z-scores for each lab, and are reported in the newest publication as percentiles of the z-score.
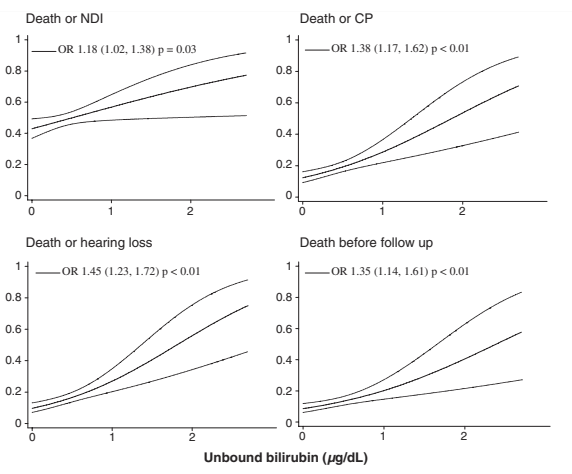
Adjusted probability plots and adjusted odds ratio (95% CI) for unbound bilirubin versus proportion of death or NDI, death or CP, death or hearing loss, and death before follow-up in clinically stable and unstable infant
But a correction published 3 years later reveals that they actually show the UB divided by 0.3 “we have standardized the unbound bilirubin by dividing the actual values by the standard deviations which is 0.3. The standardized values (in units) were used in the presentation of data in this figures which appear to be 0–3.0 units. The actual unbound bilirubin values are 0–0.9 mcg/dL”. I don’t understand how this “standardized” the data, it was clearly just a screw up that none of the 89 authors noticed. (I exaggerate).
You may also remember a secondary analysis published 4 years after the original manuscript Tyson JE, et al. Does aggressive phototherapy increase mortality while decreasing profound impairment among the smallest and sickest newborns? J Perinatol. 2012;32(9):677-84. In that publication they performed a subgroup analysis dividing the smaller babies into those ventilated and those who were not. Whether this was a preplanned subgroup or not is unclear; the publication states rather vaguely that they had plans “to relate the risks and benefits of AgPT to baseline risk factors including measures of severity of illness”. In that secondary analysis of a subgroup, using Bayesian analysis, they claimed to show that it was highly likely that phototherapy increased mortality among ventilated infants of 500-750 g. That analysis also shows that there was a probable decrease in mortality among non-ventilated 500-750 g babies (13% vs 25%), a probable decrease among larger babies who were ventilated (16% vs 19%), and a possible increase among larger non-ventilated babies (8% vs 6%). My interpretation of which is that the differences are very likely just random variations between groups. However, the authors of that secondary analysis were much more emphatic that phototherapy was decreasing the anti-oxidant benefits of bilirubin, and was generating oxidant injury and was increasing mortality in the smallest babies, if they were ventilated.
So why have they come back to these data now? (Arnold CC, et al. Unbound bilirubin and risk of severe neurodevelopmental impairment in extremely low birthweight newborns. Pediatr Res. 2025) The authors state that there are new concerns about lipid emulsions leading to increases in Free Fatty Acids and displacing bilirubin from albumin, leading to an increase in UB. But such concerns are not new at all, they date back to the 90’s or further. Perhaps more relevant is that a new method for measuring UB has become available, which might make it more clinically useful, and there are new statistical methods available, including the TMLE (Targeted Maximum Likelihood Estimation), which apparently uses machine learning to give conservative explanations of correlations between variables.
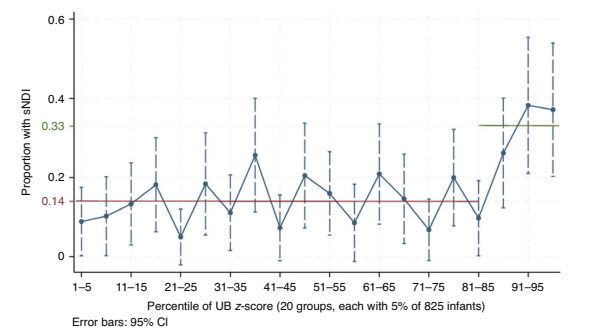
For this analysis they concentrated on “severe NDI” or sNDI, which was “based on the NDI outcomes with the strongest associations with the phototherapy regimen in the NICHD aggressive vs conservative phototherapy” LITEPOP RCT which was : a score on the Bayley II Mental or Psychomotor Developmental Index of 50 or less or a level of 5 for gross motor function (GMF), or needing bilateral hearing aids.
They divided UB into 20 slices, based on percentile of UB, as you can see from the figure below, there seems to be a threshold effect, with sNDI increased substantially for the top 15% of UB concentrations on day 5 of life.
There was very poor correlation between the total bilirubin and UB concentrations, as you can see below. But almost all of the UB concentrations associated with worse outcomes were above the threshold for phototherapy in the early treatment group, only 1 or 2 of the dots are in the upper left quadrant. You can also see, what I was not aware of previously, that far more than half of the dots are above 5 mg/dl, which implies that the phototherapy was not very effective at keeping the total bilirubin below the treatment threshold.
Most of the babies with “sNDI” did not have classic clinical signs of kernicterus, choreo-athetoid cerebral palsy, oculomotor problems, and high-tone nerve deafness. This could be because bilirubin encephalopathy is not so specific in the affected regions in very preterm infants, especially in the presence of acidosis, sepsis etc.
What should we do about this? If UB or “free” bilirubin measurement becomes more widely available, then the lack of correlation with total bilirubin strongly suggests that UB should become the variable of choice for monitoring hyperbilirubinemia in full term infants with jaundice. We could perhaps decrease the proportion of babies who get intervention while improving the prevention of kernicterus, which continues to affect somewhere around 1 in 100,000 babies, and while rare is devastating. The potential benefits among preterm infants are numerically greater, if a new trial (the UNBEATEN trial, UNbound Bilirubin EArly TreatmENt trial, I claim copyright) could show that screening for, and treating, to maintain UB < the 85%ile, improved neurological and developmental outcomes.
At the same time the trial could investigate whether the possible impact of phototherapy on mortality among the subgroup of ventilated extremely preterm infants in the NICHD trial was a real phenomenon or not.
A recurrent problem in the NICU is “bandwagon-jumping”. An intervention with some preliminary positive data, and a possible physiologic rationale is widely adopted and made part of QI bundles with little or no reliable evidence that it is either effective or safe.
One such is the hype surrounding fresh mother’s milk. There are a small number of studies showing the following impacts. (references at the end)
A reduction in laboratory indices of antioxidant activity with freezing and with refrigeration, has been shown, with the longer duration of refrigeration having a greater impact, compared to never refrigerated milk.
An impact of pasteurization, but not freezing and thawing, on Leptin concentrations, but not Adiponectin or total protein
Freezing and thawing reduce glutathione content
No impact on total fat or carbohydrate of freeze/thawing, possible increase in Free Fatty Acids.
Freezing inactivates the majority of CMV, decreasing viral load, but does not eliminate entirely
Vitamin C concentrations are reduced by refrigeration and by freezing
The effects on cellular components of refrigeration and/or freeze thawing are unclear, which is unfortunate as I suppose this is the reason that people want to give “fresh” breast milk. My literature search for this post was unable to find much data on the impacts of freezing and thawing on the endogenous cellular components of breast milk. It has been reported that the viable proportion of white cells in milk after freeze/thawing is 78% or 19%. But exactly how to determine which type of white cell is still active, is unclear to me, the most recent report I found is a brief letter with little methodological detail, which determined viability with “propidium iodide” and measured some cell markers.
And here another word of caution, what is meant by “fresh” isn’t always the same, sometimes it means never refrigerated, sometimes never frozen, sometimes not pasteurized. A recent statement from France, for example differentiates between “Raw” milk, meaning never refrigerated, and “Refrigerated” milk, with “Fresh” meaning either raw or refrigerated but never frozen. That working group developed guidelines to improve provision of raw milk, despite not presenting any clear reliable evidence of a clinical benefit.
Overall then, it seems that there is little adverse impact of freezing and thawing on macronutrients or cellular components of breast milk. There are some individual impacts, especially on vitamin C.
I guess the current enthusiasm for trying to give fresh milk must, therefore, be based on good clinical data of a benefit? (That is an ironic question, I already know the answer!) There is one cohort study (Huang J, et al. Short-term effects of fresh mother’s own milk in very preterm infants. Matern Child Nutr. 2023;19(1):e13430) comparing outcomes between babies who received “Fresh” mothers own milk, which was what the French group would call Raw milk (i.e. never refrigerated) and used within 3 hours, with the comparisons receiving pasteurized MoM. There were 170 babies <32 weeks GA in total, averaging 1150 g and 29 weeks. NEC and LOS were more frequent in the non-randomized control group, 16% and 19%, vs 10% and 7% in the controls, and there were some very small differences in feeding tolerance. The mother had to provide milk every 3 hours during the entire NICU stay.
Another Chinese cohort study (Sun H, et al. Testing the feasibility and safety of feeding preterm infants fresh mother’s own milk in the NICU: A pilot study. Sci Rep. 2019;9(1):941) compared a group of babies <30 weeks GA who received one feed a day of “Fresh” milk (unclear whether it was allowed to be refrigerated during the 4 hours that was permitted between expression and administration) to a group who received only frozen thawed milk. Infants received either MoM or donor milk (DHM), and it seems that some of the control babies could have received only DHM. There were close to 100 babies per group, averaging about 28.5 weeks gestation and some of the fresh milk babies dropped out and were not analyzed. The birth weights in the 2 groups are not mentioned, but they both, unusually, had a birthweight z score averaging about +0.3 (preterm infants usually average below 0). There was a very high rate of late onset sepsis (38%) and stage 2-3 NEC (14%) in the controls that was lower in the fresh milk group (22% and 6%).
One other study that I have seen quoted is a French database analysis which showed less BPD in NICUs that gave Fresh milk, but in that study the comparison NICUs gave pasteurized mother’s milk, as it was the recommended standard at that time in France. It also is not clear if the Fresh milk could have been frozen prior to administration or not. There was less BPD in the fresh NICUs, but no difference in NEC or in LOS, which was extremely frequent in both groups.
Although it seems attractive to some clinicians, there really is no reliable evidence that giving fresh breast milk, however it is defined, has different clinical outcomes, compared to frozen and thawed breast milk. Differences in composition are relatively minor, and impacts on cellular viability or numbers are really unclear.
The logistic implications, on the other hand, are substantial. Enabling the provision of an early fresh milk feed, daily fresh milk feeds, or exclusively fresh milk feeds, will require some resources, and organisation of those resources, to ensure that it could be done reliably and without errors in administration. A randomized controlled trial would be worthwhile to determine the true clinical impact, if any, of avoiding freeze/thawing of MoM, to see if dedicating those resources is worth it. One is planned and hopefully underway (Sun H, et al. A randomized controlled trial protocol comparing the feeds of fresh versus frozen mother’s own milk for preterm infants in the NICU. Trials. 2020;21(1):170), until the results are available, the potential benefits of Fresh, compared to Frozen and thawed, maternal breast milk must be considered Not Proven.
References (in chronologic order, most recent first)
I ran out of energy in trying to add all the hyperlinks to the references, but I guess if you care you can easily find them, all available through PubMed.
I have written frequently about my concerns with “NDI” as an important measure of neonatal outcomes, indeed, it seems to be often thought of as if it were the only important measure. It has very often been included as part of a composite outcome measure “death or NDI”.
So why am I disturbed about the use of NDI as a primary outcome measure? NDI is itself already a composite measurement, including some indicator of delayed development (most commonly one of the various iterations of the Bayley Scales of Infant Development), some severity of motor disorder expected to be permanent, i.e. Cerebral Palsy, some severity of hearing loss, and some severity of visual impairment. It was a composite invented by neonatologists and follow up specialists as a way of trying to quantify the impacts of adverse cerebral impacts of prematurity. There are many problems with this, both in the actual importance of each component of NDI, and also in the permanence of the finding. For example, most infants with low scores on developmental screening tests at 2 years do not have intellectual impairment at follow up. In the follow up of the CAP trial, for example, only 18% of babies who had a low Bayley score at 18 months (version 2 MDI <70) actually had a low IQ at 5 years (WPSII <70). This is unlike CP, for which a diagnosis at 2 years is very accurate (not 100%, but appears to be about 95% PPV) as a predictor of long term motor dysfunction, but the severity of the problem can vary, especially after a diagnosis at 2 to 3 years, where about 1/3 of infants will change their classification on the GMFCS, either to a higher or a lower score. Visual and auditory impairments seem to be more permanent and invariable, but are a much smaller part of the NDI.
And, of course, combining NDI with death as part of a composite outcome implies that they are equally important, and means that an intervention which decreases death may not be found to be significant is there is an increase in low BSID scores in the survivors (for example).
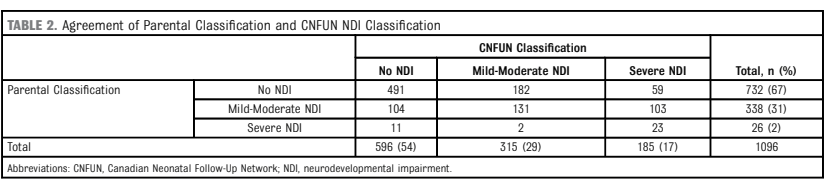
Do parents of babies who are labelled as having NDI think that their infants are impaired? That is the question asked in a new publication from the follow up centres across Canada (Canadian Neonatal Follow-Up Network, CNFUN). Richter LL, et al. Parental and Medical Classification of Neurodevelopment in Children Born Preterm. Pediatrics. 2025. Over 1000 very preterm infants are involved in the study, and their parents were asked if they thought that their child had a developmental impairment when they attended a follow-up clinic appointment, but before they completed the standardised evaluation. They then had their evaluation and were classified as having no NDI or :
“to have a mild-moderate NDI if they had any 1 or more of the following: CP with GMFCS 1 or 2; Bayley-III motor, cognitive, or language composite scores 70 to 84; hearing loss without requirement for hearing devices or unilateral visual impairment. A child was considered to have a severe NDI if they had any 1 or more of the following: CP with GMFCS 3, 4, or 5; Bayley-III motor, cognitive or language composite scores <70; hearing aid or cochlear implant; or bilateral visual impairment.”
As this table shows, there was poor agreement between what the parents thought, and what the standardised evaluation stated. Most of the disagreements were parents considering their infants to not be impaired, or to be less impaired than the standard classification. There were 185 infants with “severe NDI” according to the definition above, only 23 parents thought their child was severely impaired, in contrast, among the 596 with no NDI, there were 11 parents who found their child to have severe impairment, and 104 thought they had mild-moderate impairment.
Some of the details of the analyses are quite interesting, for example, the small number of infants with serious CP, GMFCS 4 or 5, were mostly considered to have moderate or severe impairment by parents. The cognitive scores of infants who agreed that their infant, with CNFUN defined severe NDI, had at least moderate impairment were lower (median 70) than those who disagreed (median 80).
Many problems faced by families with ex-preterm infants are not captured by “NDI”. This is reflected, I think, by those parents who thought their child was impaired despite not satisfying CNFUN definitions, such infants were much more likely to be using technology at home, and more likely to have been referred for occupational therapy, or to see a psychologist or other therapist. Needing re-hospitalisation also made parent more likely to agree that their infant had an impairment.
Because we haven’t measured some of the things that impact families, such as behavioural disturbances, feeding problems, and sleep disruption, we really don’t know if they are affected by any of our NICU interventions. It wouldn’t surprise me if some interventions, ranging from postnatal steroids to skin-to-skin care or light cycling, might have major impacts on those outcomes. We just don’t know.
What should we do about findings such as these newly published data, and others from the Parents’ Voices project? Defining a single ‘yes or no’ outcome variable is the old-fashioned way of designing research and determining the benefit of an intervention. There are much better ways of comparing outcomes between groups, ways which can take into account the variety of outcomes, and the preferences of parents. It takes some extra work to define the kind of ordinal outcomes which reflect the values of parents and the relative importance of each component, but that is hugely preferable to using composite outcomes which implicitly value each component as being equivalent. Being dead, having a Bayley Cognitive composite of 69, having severe visual loss all qualify as “dead or severe NDI”, but the implications are enormously different.
In the future outcomes we measure should focus on how infants function, and should recognize that the answer to the question “how is your child doing?” is not a dichotomous choice.
Just back from a week in Panama, organised by “Wings“, mostly in Darién province at the extreme east of the country. A really amazing experience, with over 300 bird species seen, including just over 200 “lifers” for me. On my other blog, I have posted several posts, a trip report with many photos.
As a taster, this is a Collared Aracari, and below King Vultures.