
In this observational study, the authors recorded sleep architecture overnight shortly prior to discharge of 76 preterm infants, averaging 30 weeks GA.
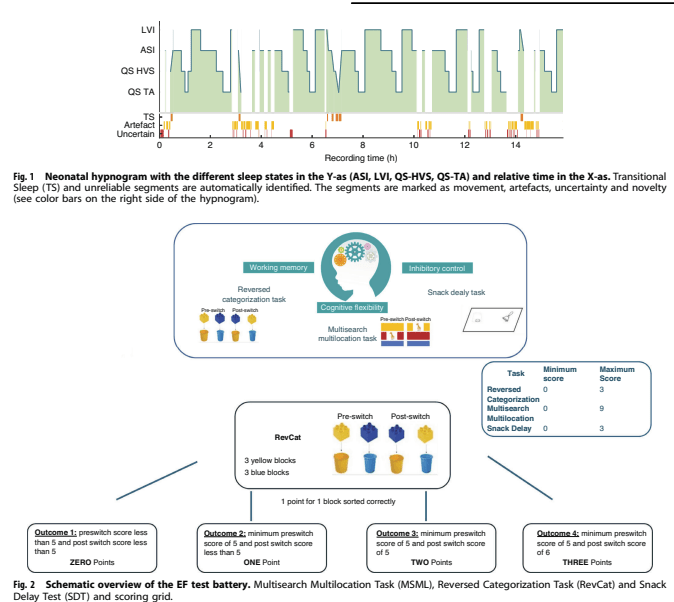
The main finding was that infants with less sleep time (as a percentage of the recording) had more executive function problems. This was a single recording prior to discharge, and might not reflect total sleep problems during the hospitalisation, but is certainly suggestive that preterms need their sleep.
Take Home Message : Sleep may be important for development of normal executive function among preterm infants.
In this randomized study from our institution, my colleagues randomized simulated intubations by residents to having a lot of stress, which included an attending staff running into the room and breathing over their shoulder, they also had alarm and background noise, a nurse and an RT in attendance, and the manikin desaturated. The low stress simulation had no noise, a low fidelity manikin that couldn’t desaturate, and fewer personnel.
They showed that they were able to stress the trainees, as their heart rates went up more in the high-stress group, but that didn’t have an impact on success or time to intubation. Maybe that has something to do with an overall supportive and positive environment in our institution, trainees know that even if a procedure goes badly they won’t be yelled at! They also knew that no manikin would be seriously harmed in the making of this study.
Take Home Message : in a simulated intubation, more stressful situation did not impact competency.
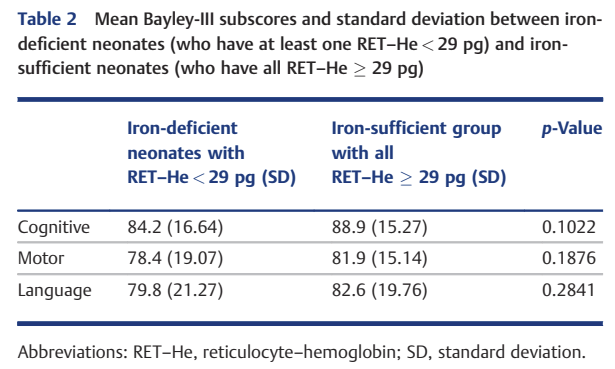
The measure of iron deficiency that the Utah group was investigating here was new to me. The average haemoglobin content in a reticulocyte (RET-He) is apparently one of the best ways of determining iron status, and has been shown in animal models to correlated with brain iron deficiency. The value should stay over 29 pg, it seems. There are good data from full term infants, that iron deficiency has impacts on neurodevelopment, including on executive function; but little similar data from the preterm. This observational study of very preterm infants <28 weeks GA compared Bayley version 3 scores at 2 years corrected age in 78 infants who were left after exclusions (of receiving erythropoietin or an analogue, being in a trial of EPO, or not having an RET-He measured).
There was no significant difference in scores between the babies who had at least one RET-He <29 and those in whom all the measured values were >29, but looking at the table, all the mean scores were higher in the babies without evidence of iron deficiency.
The correlation of average daily Fe dose with the Bayley cognitive score was statistically significant, but not very impressive.
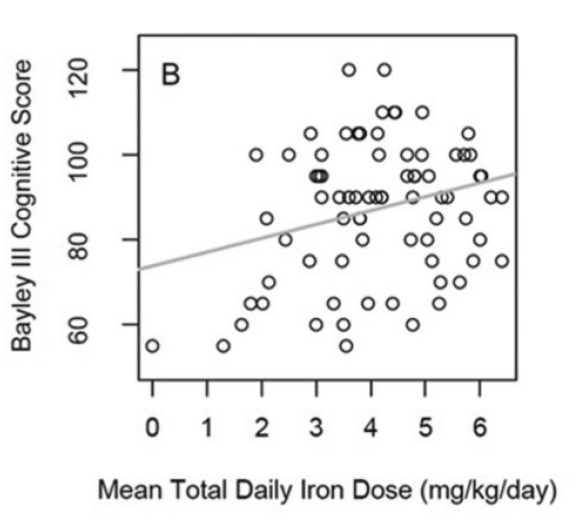
But, there are so many influences on cognitive development in very preterm infants that are not directly related to iron intake or iron status, such as growth restriction, lung injury, infections, intermittent hypoxia, social status, number of books in the home, and maternal education. With this in mind, to find even a weak correlation, and a minor difference in Bayley scores is highly suggestive to me. The median daily Fe dose was 4.4 mg/kg/d (IQR 3.2-5.6) I was surprised to see that the range included a baby with a dose of 0 (!).
One concern I have about this paper is that the babies were born 2014-2018, and the latest follow up included was in 2020. I don’t know why there aren’t any infants from the last 6 years, but the babies benefited from delayed cord clamping, which, of course, increases initial iron stores.
The recommended range of iron intakes from ESPGHAN is 2-3 mg/kg/d, but that is based on no data about neurodevelopmental outcome in the very preterm. There is one study in late preterm infants which showed improved outcomes with iron supplementation compared to no supplementation, but the Systematic Reviews available (the latest Cochrane review is from 2012) include almost no information on the very preterm. The most recent SR that I found is from 2022, the authors restricted the studies to those with babies receiving human milk, and found only 3 RCTs comparing different doses of iron. Those 3 trials included a tiny number of babies, about 140 infants total, and only one of them had some follow up, which on post hoc testing showed a decrease in adverse motor outcomes (BSID II PDI score <85) in the higher dose group.
I was a bit surprised how little data we have on which to base the dose of iron that we give to our very preterm babies. It seems to me that it would be an easy study to design fund and perform. If simply increasing the standard dose of iron will improve developmental outcomes without having any adverse impact, that would have a major impact on a very easily performed intervention. Of note the little data currently available shows no increase in adverse outcomes with higher dose iron compared to a standard 2 mg/kg/d.
Take Home Message : the current standard dose of enteral iron supplement may be insufficient, but the data to support any dose are lacking. Probably, for now, the standard should be 3 mg/kg/d. More studies are desperately needed.






